Department of Pediatric Hematology, Immunology and Infectious Diseases, Emma Children's Hospital, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Eur Radiol. 2020 Jan;30(1):432-441. doi: 10.1007/s00330-019-06367-6. Epub 2019 Aug 19.
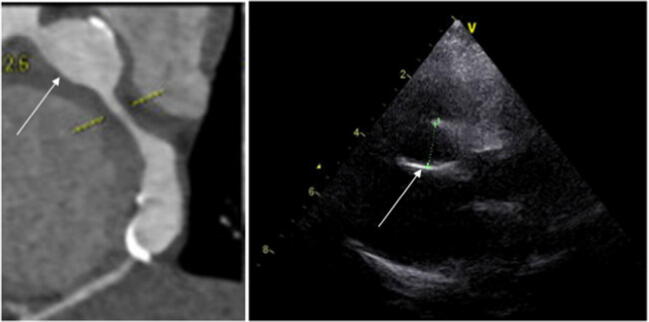
Kawasaki disease (KD) is a vasculitis with formation of coronary artery aneurysms (CAAs) that can lead to myocardial ischemia. Echocardiography is the primary imaging modality for the coronary arteries despite limited visualization. Coronary angiography (CAG) is the gold standard yet invasive with high-radiation exposure. To date however, state-of-the-art CT scanners enable high-quality low-dose coronary computed tomographic angiography (cCTA) imaging. The aim of our study in KD is to report (i) the diagnostic yield of cCTA compared to echocardiography, and (ii) the radiation dose.
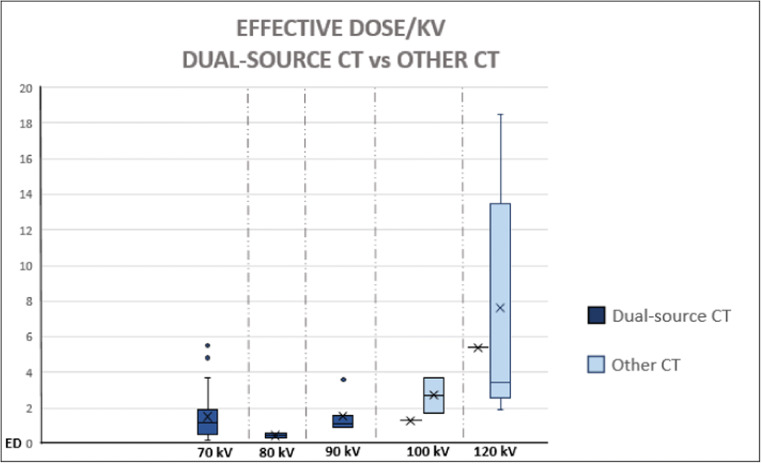
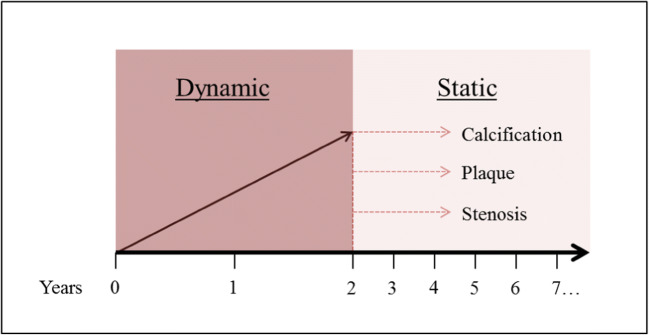
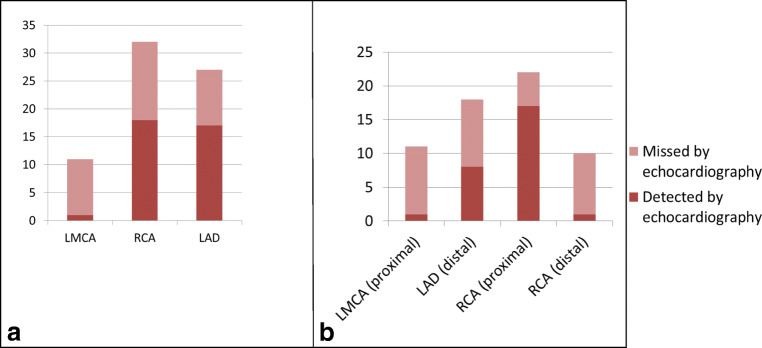
We collected data of KD patients who underwent cCTA. cCTA findings were compared with echocardiography results. In 70 KD patients (median age 15.1 years [0.5-59.5 years]; 78% male; 38% giant CAA), the cCTA identified 61 CAAs, of which 34 (56%, with a Z score > 3, in 22 patients) were not detected by echocardiography. In addition, the left circumflex (aneurysmatic in 6 patients) was always visible upon cCTA and not detected upon echocardiography. Calcifications, plaques, and/or thrombi were visualized by cCTA in 25 coronary arteries (15 patients). Calcifications were seen as early as 2.7 years after onset of disease. In 5 patients, the cCTA findings resulted in an immediate change of treatment. The median effective dose (ED) in millisievert differed significantly (p < 0.01) between third-generation dual-source and other CT scanners (1.5 [0.3-9.4] (n = 56) vs 3.8 [1.7-20.0] (n = 14)).
The diagnostic yield of third-generation dual-source cCTA combined with reduced radiation exposure makes cCTA a favorable diagnostic modality to complete the diagnosis and long-term treatment indications for KD.
• cCTA is a favorable diagnostic modality to complete the diagnosis and long-term treatment indications for Kawasaki disease. • Kawasaki disease patients with proven coronary artery involvement on echocardiography require additional imaging.
川崎病(KD)是一种血管炎,可导致冠状动脉瘤(CAA)形成,进而导致心肌缺血。尽管超声心动图对冠状动脉的可视化程度有限,但它仍是主要的影像学检查方法。冠状动脉造影(CAG)是金标准,但具有侵袭性且辐射暴露量高。然而,迄今为止,最先进的 CT 扫描仪能够实现高质量的低剂量冠状动脉计算机断层血管造影(cCTA)成像。我们研究川崎病的目的是报告:(i)cCTA 与超声心动图相比的诊断效果,以及(ii)辐射剂量。
我们收集了接受 cCTA 的川崎病患者的数据。将 cCTA 结果与超声心动图结果进行比较。在 70 例川崎病患者(中位数年龄 15.1 岁[0.5-59.5 岁];78%为男性;38%为巨大 CAA)中,cCTA 发现了 61 个 CAA,其中 34 个(56%,Z 评分>3,22 例患者)未被超声心动图发现。此外,左回旋支(6 例患者的动脉瘤)在 cCTA 上始终可见,而在超声心动图上不可见。25 支冠状动脉(15 例患者)可见钙化、斑块和/或血栓。早在疾病发病后 2.7 年即可发现钙化。在 5 例患者中,cCTA 的检查结果导致了治疗方案的立即改变。以毫西弗为单位的有效剂量(ED)在第三代双源 CT 与其他 CT 扫描仪之间差异有统计学意义(p<0.01)(56 例[1.5[0.3-9.4] vs 14 例[3.8[1.7-20.0])。
第三代双源 cCTA 联合低辐射剂量的诊断效果较好,使 cCTA 成为一种理想的诊断方法,可用于完成川崎病的诊断和长期治疗指征。
• cCTA 是一种理想的诊断方法,可用于完成川崎病的诊断和长期治疗指征。• 经超声心动图证实有冠状动脉受累的川崎病患者需要进一步影像学检查。