Université de Paris, Centre of Research in Epidemiology and Statistics, INSERM, Institut national de la recherche agronomique, Paris, France.
APHP, Unité de Recherche Clinique, Hôpitaux Universitaires Paris île-de-France Ouest, Paris, France.
PLoS Med. 2019 Aug 20;16(8):e1002871. doi: 10.1371/journal.pmed.1002871. eCollection 2019 Aug.
Weight-control interventions in pregnant women with overweight or obesity have limited effectiveness for fetal growth and birth outcomes. Interventions or prevention programs aiming at the pre-pregnancy period should be considered. However, how the woman's weight change before pregnancy affects fetal growth is not known. We investigated the association between weight change over the year before pregnancy and birth weight.
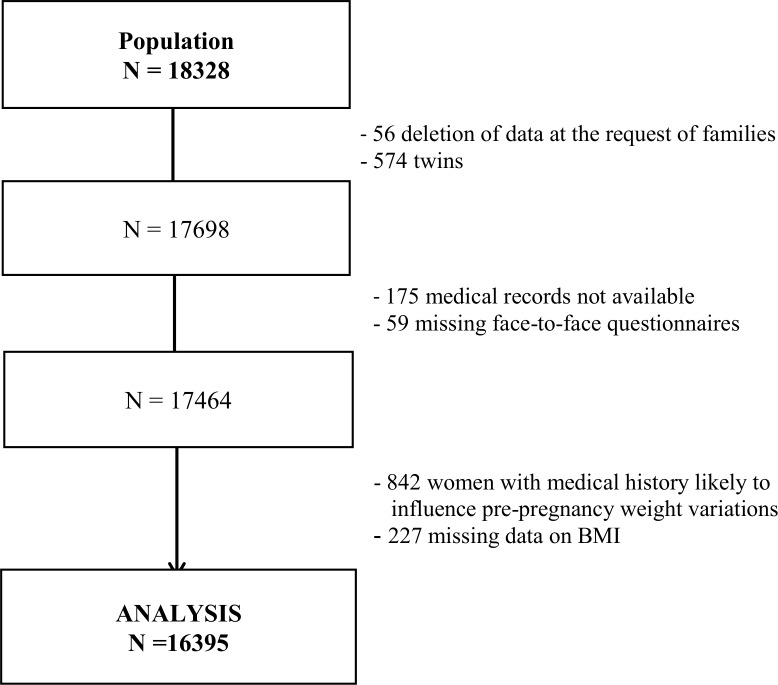
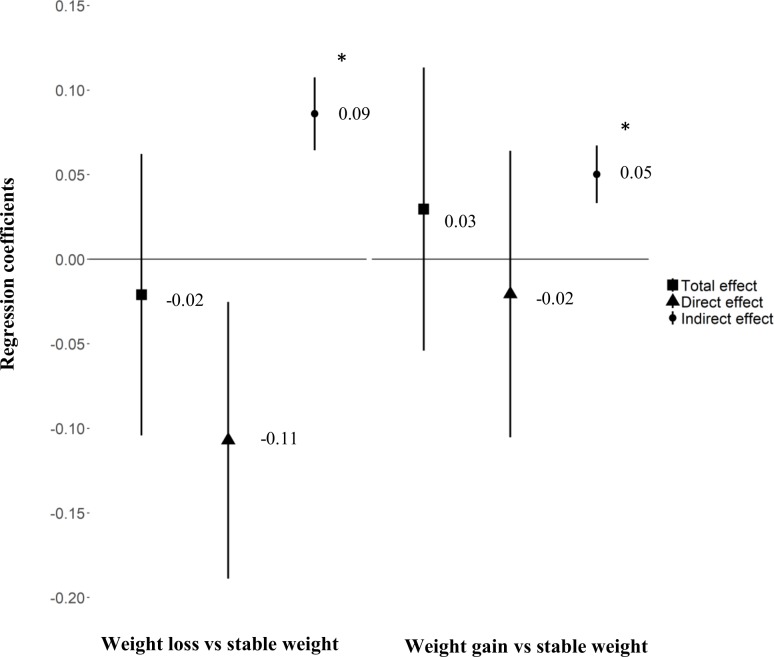
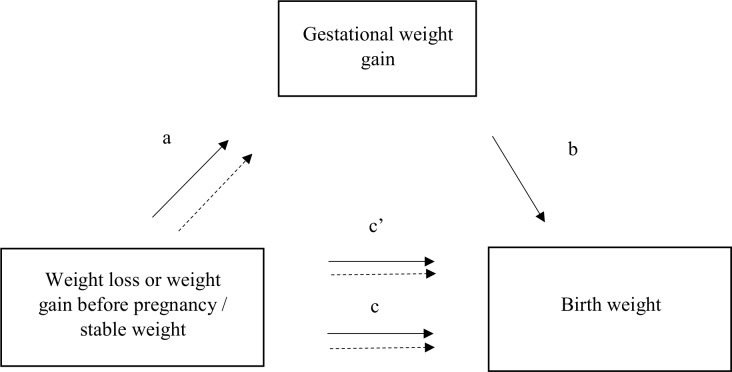
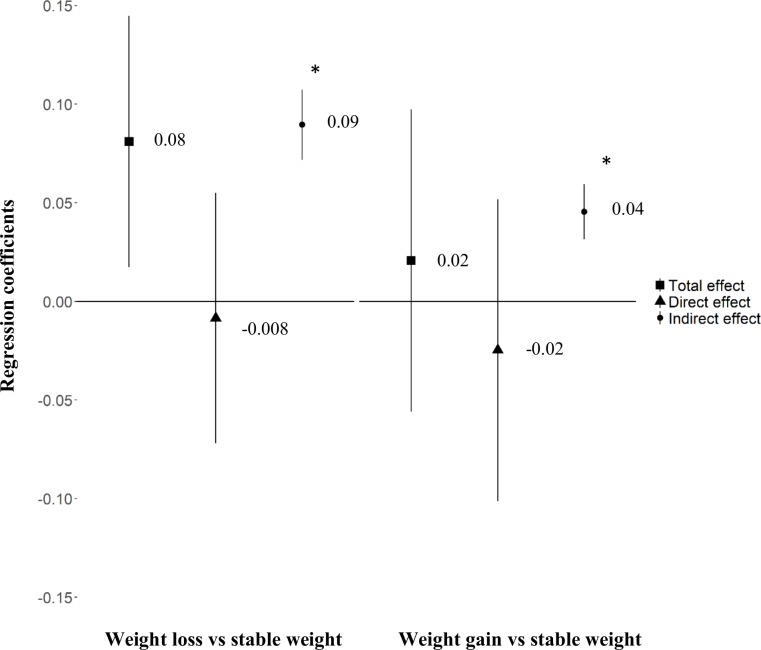
We used the inclusion data of 16,395 women from the ELFE French national birth cohort, a nationally representative cohort in which infants were enrolled at birth with their families in 2011. Maternal weight change was self-reported and classified into 3 groups: moderate weight variation or stable weight, weight loss > 5 kg, and weight gain > 5 kg or both weight loss and gain > 5 kg. Multiple linear regression models were used to investigate the association between pre-pregnancy weight change and a birth weight z-score calculated according to the French Audipog reference, adjusted for a large set of maternal characteristics. The analyses were stratified by maternal body mass index (BMI) at conception (<25 versus ≥25 kg/m2) and adjusted for BMI within these categories. We used the MacKinnon method to test the mediating effect of gestational weight gain (GWG) on these associations. Mother's mean age was 30.5 years, 87% were born in France, and 26% had overweight or obesity. For women in either BMI category at conception, GWG was more than 2 kg higher, on average, for women with weight loss before pregnancy than for women with stable weight or moderate weight variation. For women with BMI < 25 kg/m2 at conception, birth weight was significantly higher with weight loss than stable weight before pregnancy (β = 0.08 [95% CI 0.02; 0.14], p = 0.01), and this total effect was explained by a significant mediating effect through GWG. For women with BMI ≥ 25 kg/m2 at conception, birth weight was not associated with pre-pregnancy weight loss during the year before pregnancy. Mediation analysis revealed that in these women, the direct effect of pre-pregnancy weight loss that would have resulted in a smaller birth weight z-score (β = -0.11 [95% CI -0.19; -0.03], p = 0.01) was cancelled out by the GWG. The mediating effect of GWG was even higher when weight loss resulted from a restrictive diet in the year before pregnancy. Weight gain before pregnancy was not associated with birth weight. Although we included a large number of women and had extensive data, the only potential cause of pre-pregnancy weight loss that was investigated was dieting for intentional weight loss. We have no information on other potential causes but did however exclude women with a history of pre-pregnancy chronic disease. Another limitation is declaration bias due to self-reported data.
Health professionals should be aware that GWG may offset the expected effect of weight loss before conception on fetal growth in overweight and obese women. Further studies are required to understand the underlying mechanisms in order to develop weight-control interventions and improve maternal periconceptional health and developmental conditions for the fetus.
针对超重或肥胖孕妇的体重控制干预措施对胎儿生长和出生结局的效果有限。应考虑针对孕前阶段的干预措施或预防计划。然而,孕妇在怀孕前体重的变化如何影响胎儿生长尚不清楚。我们研究了孕前一年体重变化与出生体重之间的关系。
我们使用了来自法国 ELFE 全国出生队列的 16395 名女性的纳入数据,这是一个全国代表性的队列,在 2011 年在婴儿出生时及其家庭一起入组。孕妇体重变化是自我报告的,并分为 3 组:体重适度变化或稳定,体重减轻>5 公斤,以及体重增加>5 公斤或体重减轻和增加>5 公斤。使用多元线性回归模型来研究孕前体重变化与根据法国 Audipog 参考值计算的出生体重 z 评分之间的关联,该模型根据大量的产妇特征进行了调整。根据受孕时的母体 BMI(<25 与≥25kg/m2)对分析进行分层,并对这些类别中的 BMI 进行了调整。我们使用 MacKinnon 方法来检验 GWG 对这些关联的中介作用。母亲的平均年龄为 30.5 岁,87%出生在法国,26%超重或肥胖。对于受孕时 BMI 处于任一类别中的女性,与体重稳定或体重适度变化的女性相比,孕前体重减轻的女性平均 GWG 增加了 2 公斤以上。对于受孕时 BMI<25kg/m2 的女性,与孕前体重稳定相比,体重减轻与出生体重显著增加(β=0.08[95%CI 0.02;0.14],p=0.01),并且这种总效应通过 GWG 产生了显著的中介作用。对于受孕时 BMI≥25kg/m2 的女性,孕前体重减轻与出生体重无关。中介分析表明,在这些女性中,孕前体重减轻导致的出生体重 z 评分较小的直接效应(β=-0.11[95%CI-0.19;-0.03],p=0.01)被 GWG 抵消。当孕前体重减轻是由于饮食限制时,GWG 的中介作用甚至更高。孕前体重增加与出生体重无关。尽管我们纳入了大量女性并拥有广泛的数据,但孕前体重减轻的唯一潜在原因是为了有意减轻体重而节食。我们没有其他潜在原因的信息,但我们确实排除了有孕前慢性疾病史的女性。另一个限制是由于自我报告数据而导致的申报偏差。
卫生专业人员应该意识到,GWG 可能会抵消超重和肥胖女性孕前体重减轻对胎儿生长的预期影响。需要进一步研究以了解潜在机制,以便制定体重控制干预措施并改善孕妇围孕期健康和胎儿发育状况。