Department of Health Research and Policy, Stanford University School of Medicine, Stanford, California, United States of America.
PIVOT, Ranomafana, Madagascar.
PLoS Med. 2019 Aug 20;16(8):e1002869. doi: 10.1371/journal.pmed.1002869. eCollection 2019 Aug.
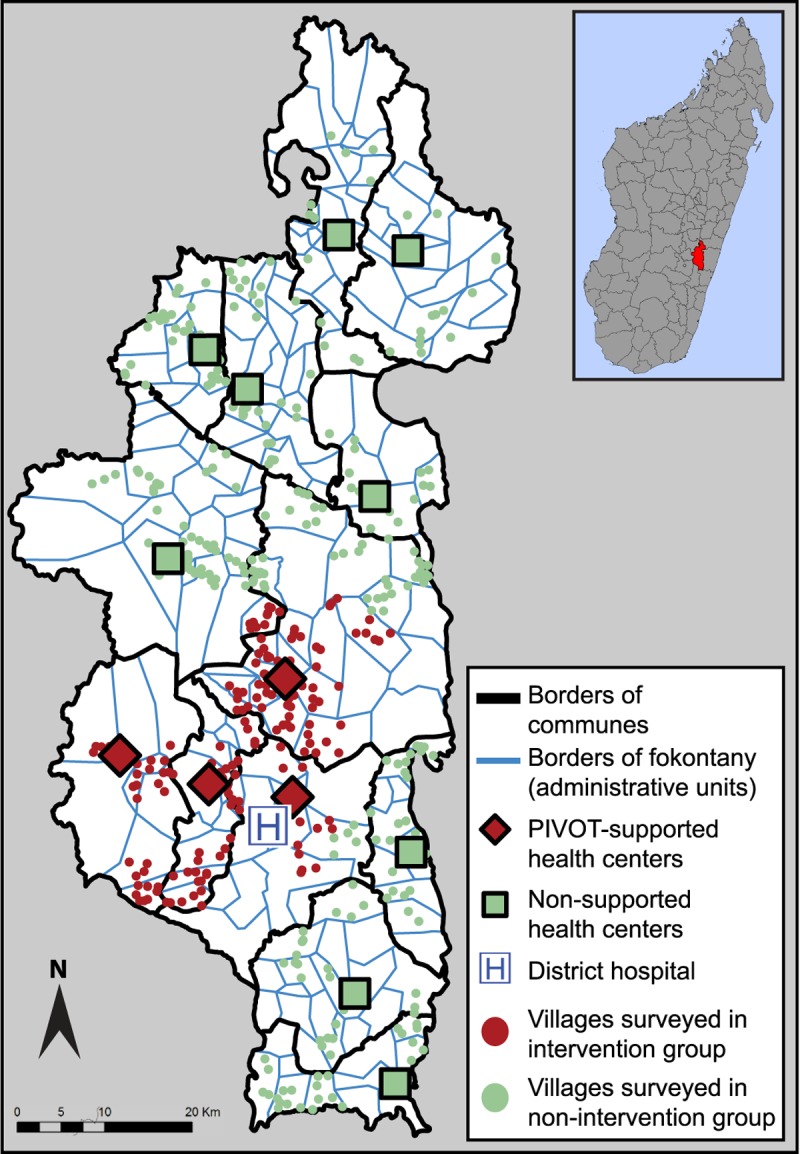
In order to reach the health-related Sustainable Development Goals (SDGs) by 2030, gains attained in access to primary healthcare must be matched by gains in the quality of services delivered. Despite the broad consensus around the need to address quality, studies on the impact of health system strengthening (HSS) have focused predominantly on measures of healthcare access. Here, we examine changes in the content of maternal and child care as a proxy for healthcare quality, to better evaluate the effectiveness of an HSS intervention in a rural district of Madagascar. The intervention aimed at improving system readiness at all levels of care (community health, primary health centers, district hospital) through facility renovations, staffing, equipment, and training, while removing logistical and financial barriers to medical care (e.g., ambulance network and user-fee exemptions).
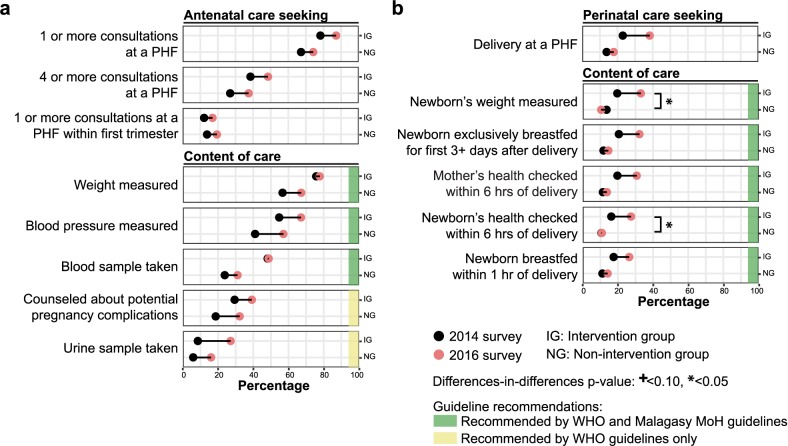
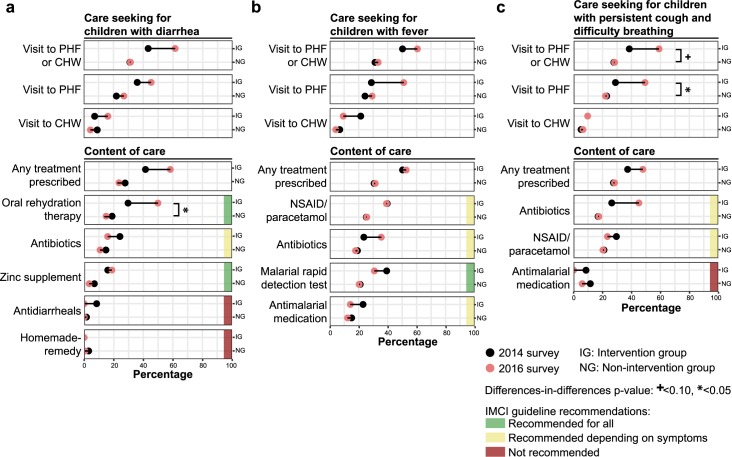
We carried out a district-representative open longitudinal cohort study, with surveys administered to 1,522 households in the Ifanadiana district of Madagascar at the start of the HSS intervention in 2014, and again to 1,514 households in 2016. We examined changes in healthcare seeking behavior and outputs for sick-child care among children <5 years old, as well as for antenatal care and perinatal care among women aged 15-49. We used a difference-in-differences (DiD) analysis to compare trends between the intervention group (i.e., people living inside the HSS catchment area) and the non-intervention comparison group (i.e., the rest of the district). In addition, we used health facility-based surveys, monitoring service availability and readiness, to assess changes in the operational capacities of facilities supported by the intervention. The cohort study included 657 and 411 children (mean age = 2 years) reported to be ill in the 2014 and 2016 surveys, respectively (27.8% and 23.8% in the intervention group for each survey), as well as 552 and 524 women (mean age = 28 years) reported to have a live birth within the previous two years in the 2014 and 2016 surveys, respectively (31.5% and 29.6% in the intervention group for each survey). Over the two-year study period, the proportion of people who reported seeking care at health facilities experienced a relative change of +51.2% (from 41.4% in 2014 to 62.5% in 2016) and -7.1% (from 30.0% to 27.9%) in the intervention and non-intervention groups, respectively, for sick-child care (DiD p-value = 0.01); +11.4% (from 78.3% to 87.2%), and +10.3% (from 67.3% to 74.2%) for antenatal care (p-value = 0.75); and +66.2% (from 23.1% to 38.3%) and +28.9% (from 13.9% to 17.9%) for perinatal care (p-value = 0.13). Most indicators of care content, including rates of medication prescription and diagnostic test administration, appeared to increase more in the intervention compared to in the non-intervention group for the three areas of care we assessed. The reported prescription rate for oral rehydration therapy among children with diarrhea changed by +68.5% (from 29.6% to 49.9%) and -23.2% (from 17.8% to 13.7%) in the intervention and non-intervention groups, respectively (p-value = 0.05). However, trends observed in the care content varied widely by indicator and did not always match the large apparent increases observed in care seeking behavior, particularly for antenatal care, reflecting important gaps in the provision of essential health services for individuals who sought care. The main limitation of this study is that the intervention catchment was not randomly allocated, and some demographic indicators were better for this group at baseline than for the rest of the district, which could have impacted the trends observed.
Using a district-representative longitudinal cohort to assess the content of care delivered to the population, we found a substantial increase over the two-year study period in the prescription rate for ill children and in all World Health Organization (WHO)-recommended perinatal care outputs assessed in the intervention group, with more modest changes observed in the non-intervention group. Despite improvements associated with the HSS intervention, this study highlights the need for further quality improvement in certain areas of the district's healthcare system. We show how content of care, measured through standard population-based surveys, can be used as a component of HSS impact evaluations, enabling healthcare leaders to track progress as well as identify and address specific gaps in the provision of services that extend beyond care access.
为了在 2030 年之前实现与健康相关的可持续发展目标 (SDG),必须在获得初级医疗保健方面取得的成果与提供服务的质量方面取得的成果相匹配。尽管人们普遍认为需要解决质量问题,但有关卫生系统强化 (HSS) 影响的研究主要集中在医疗保健可及性的衡量指标上。在这里,我们检查了母婴保健内容的变化,作为医疗保健质量的替代指标,以更好地评估农村地区的 HSS 干预措施的有效性。该干预措施旨在通过设施翻新、人员配备、设备和培训来提高各级医疗保健服务的准备就绪程度(社区卫生、初级保健中心、地区医院),同时消除医疗保健服务(如救护车网络和免除用户费用)的后勤和财务障碍。
我们进行了具有代表性的地区纵向队列研究,在 2014 年 HSS 干预开始时对马达加斯加伊法纳迪纳区的 1522 户家庭进行了调查,并于 2016 年再次对 1514 户家庭进行了调查。我们调查了 5 岁以下儿童的患病儿童护理以及 15-49 岁妇女的产前护理和围产期护理的医疗保健寻求行为和产出的变化。我们使用差异中的差异 (DiD) 分析来比较干预组(即居住在 HSS 集水区内的人)和非干预对照组(即该地区的其余部分)之间的趋势。此外,我们还使用了基于卫生设施的调查,监测服务的可用性和准备情况,以评估干预措施支持的设施的运营能力的变化。该队列研究包括 657 名和 411 名儿童(平均年龄为 2 岁)报告在 2014 年和 2016 年的调查中生病(每个调查中干预组的比例分别为 27.8%和 23.8%),以及 552 名和 524 名妇女(平均年龄为 28 岁)报告在过去两年中有活产(每个调查中干预组的比例分别为 31.5%和 29.6%)。在为期两年的研究期间,报告在卫生设施寻求医疗保健的人数比例发生了相对变化+51.2%(从 2014 年的 41.4%到 2016 年的 62.5%)和-7.1%(从 30.0%到 27.9%)在干预组和非干预组中,分别用于患病儿童护理(DiD p 值=0.01);+11.4%(从 78.3%到 87.2%)和+10.3%(从 67.3%到 74.2%)用于产前护理(p 值=0.75);和+66.2%(从 23.1%到 38.3%)和+28.9%(从 13.9%到 17.9%)用于围产期护理(p 值=0.13)。我们评估的三个护理领域中,大多数护理内容指标,包括药物处方率和诊断检测率,似乎在干预组中比在非干预组中增加得更多。报告的腹泻儿童口服补液疗法处方率增加了+68.5%(从 29.6%到 49.9%)和-23.2%(从 17.8%到 13.7%),分别在干预组和非干预组中(p 值=0.05)。然而,我们观察到的护理内容趋势差异很大,并且并不总是与我们观察到的护理寻求行为的明显增加相匹配,特别是对于产前护理,这反映了为寻求医疗保健的个人提供基本卫生服务方面存在重要差距。本研究的主要限制是干预集水区不是随机分配的,并且该组的一些人口指标在基线时比该地区的其他地区要好,这可能会影响观察到的趋势。
使用具有代表性的地区纵向队列来评估向人群提供的护理内容,我们发现,在为期两年的研究期间,患病儿童的处方率以及世卫组织推荐的所有围产期护理产出都有大幅增加,而在非干预组中观察到的变化则更为温和。尽管与 HSS 干预相关的改进,但这项研究强调了在该地区的医疗保健系统中某些领域需要进一步提高质量。我们展示了如何通过基于标准人群的调查来衡量护理内容,作为 HSS 影响评估的一部分,使医疗保健领导者能够跟踪进展情况,以及识别和解决服务提供方面的具体差距,这些差距超出了医疗保健可及性的范围。