Health Economics Research Group, Department of Clinical Sciences, College of Health and Life Sciences, Brunel University London, Uxbridge, UK
Health Economics Research Group, Department of Clinical Sciences, College of Health and Life Sciences, Brunel University London, Uxbridge, UK.
Arch Dis Child. 2020 Feb;105(2):155-159. doi: 10.1136/archdischild-2018-316741. Epub 2019 Aug 23.
To provide the first estimate of the cost-effectiveness of financial incentive for breastfeeding intervention compared with usual care.
Within-cluster ('ward'-level) randomised controlled trial cost-effectiveness analysis (trial registration number ISRCTN44898617).
Five local authority districts in the North of England.
5398 mother-infant dyads (intervention arm), 4612 mother-infant dyads (control arm).
Offering a financial incentive (over a 6-month period) on breast feeding to women living in areas with low breastfeeding prevalence (<40% at 6-8 weeks).
Babies breast fed (receiving breastmilk) at 6-8 weeks, and cost per additional baby breast fed.
Costs were compared with differences in area-level data on babies' breast fed in order to estimate a cost per additional baby breast fed and the quality-adjusted life year (QALY) gains required over the lifetime of babies to justify intervention cost.
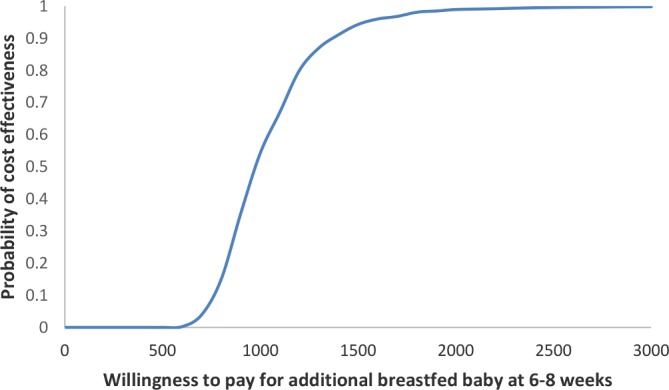
In the trial, the total cost of providing the intervention in 46 wards was £462 600, with an average cost per ward of £9989 and per baby of £91. At follow-up, area-level breastfeeding prevalence at 6-8 weeks was 31.7% (95% CI 29.4 to 34.0) in control areas and 37.9% (95% CI 35.0 to 40.8) in intervention areas. The adjusted difference between intervention and control was 5.7 percentage points (95% CI 2.7 to 8.6; p<0.001), resulting in 10 (95% CI 6 to 14) more additional babies breast fed in the intervention wards (39 vs 29). The cost per additional baby breast fed at 6-8 weeks was £974. At a cost per QALY threshold of £20 000 (recommended in England), an additional breastfed baby would need to show a QALY gain of 0.05 over their lifetime to justify the intervention cost. If decision makers are willing to pay £974 (or more) per additional baby breast fed at a QALY gain of 0.05, then this intervention could be cost-effective. Results were robust to sensitivity analyses.
This study provides information to help inform public health guidance on breast feeding. To make the economic case unequivocal, evidence on the varied and long-term health benefits of breast feeding to both the baby and mother and the effectiveness of financial incentives for breastfeeding beyond 6-8 weeks is required.
提供母乳喂养干预经济激励措施的成本效益的首次估计,与常规护理相比。
集群内(“病房”级)随机对照试验成本效益分析(试验注册号 ISRCTN44898617)。
英格兰北部的五个地方当局区。
5398 名母婴对(干预组),4612 名母婴对(对照组)。
为母乳喂养率低的地区(6-8 周时<40%)的妇女提供母乳喂养的经济激励(6 个月期间)。
6-8 周时婴儿母乳喂养情况,以及每增加一名婴儿母乳喂养的成本。
通过比较区域水平数据中婴儿母乳喂养情况的差异来比较成本,以估计干预成本所需的每增加一名婴儿母乳喂养的成本和终生获得的质量调整生命年(QALY)收益。
在试验中,46 个病房提供干预措施的总费用为 462600 英镑,每个病房的平均费用为 9989 英镑,每个婴儿的费用为 91 英镑。在随访时,控制区 6-8 周时母乳喂养率为 31.7%(95%CI 29.4 至 34.0),干预区为 37.9%(95%CI 35.0 至 40.8)。干预组和对照组之间的调整差异为 5.7 个百分点(95%CI 2.7 至 8.6;p<0.001),干预病房中额外母乳喂养的婴儿增加了 10 名(95%CI 6 至 14 名)(39 名比 29 名)。6-8 周时每增加一名婴儿母乳喂养的成本为 974 英镑。在 20000 英镑/QALY (英格兰推荐)的成本效益阈值下,需要额外的母乳喂养婴儿在其一生中获得 0.05 的 QALY 收益,才能证明干预成本的合理性。如果决策者愿意为每增加一名婴儿母乳喂养支付 974 英镑(或更多),在获得 0.05 的 QALY 收益的情况下,那么这种干预措施可能具有成本效益。结果对敏感性分析具有稳健性。
本研究提供了有助于为母乳喂养提供公共卫生指导的信息。为了明确经济情况,需要提供有关母乳喂养对婴儿和母亲的各种长期健康益处以及经济激励措施对 6-8 周以后母乳喂养的有效性的证据。