Moreno Juste Aida, Menditto Enrica, Orlando Valentina, Monetti Valeria Marina, Gimeno Miguel Antonio, González Rubio Francisca, Aza-Pascual-Salcedo María Mercedes, Cahir Caitriona, Prados Torres Alexandra, Riccardi Gabriele
EpiChron Research Group, Aragon Health Sciences Institute (IACS), IIS Aragon, REDISSEC ISCIII. Miguel Servet University Hospital, Zaragoza, Spain.
Aragon Health Service (SALUD), Department III of Zaragoza, Zaragoza, Spain.
Front Pharmacol. 2019 Aug 6;10:870. doi: 10.3389/fphar.2019.00870. eCollection 2019.
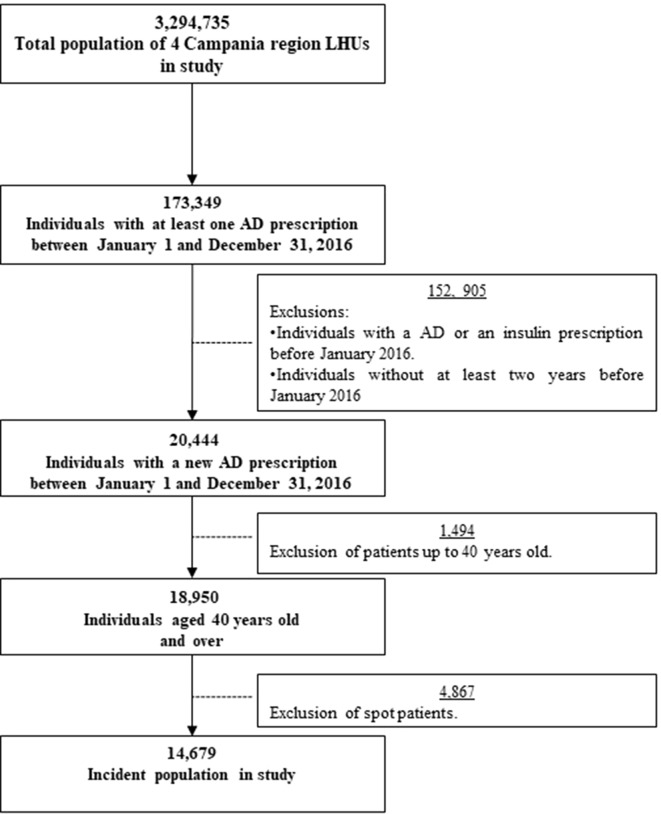
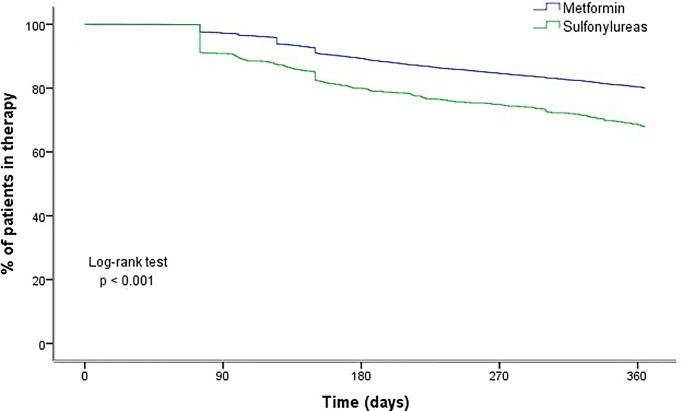
The steady increase in type 2 diabetes prevalence and the availability of new antidiabetic drugs (AD) have risen the use of these drugs with a change in the patterns of specific drug utilization. The complexity of this treatment is due to successive treatment initiation, switching and addition in order to maintain glycaemic control. The aim of this study was to describe the utilization patterns of ADs at initiation, treatment addition, and switching profiles and to measure factors influencing persistence to therapy. Retrospective observational study. Data were retrieved from the Campania Regional Database for Medication Consumption. Population consisted of patients receiving at least one prescription of ADs between January 1 and December 31, 2016. We calculated time to treatment switching or add-on as median number of days and interquartile range (IQR). Persistence rates were estimated using the Kaplan-Meier method. We used Cox regression models to estimate the likelihood of non-persistence over 1 year of follow-up. Hazard ratios and 95% confidence intervals were calculated. Of 14,679 patients, 86.9% started with monotherapy and 13.1% with combination therapy. Most common initial treatment was metformin in both monotherapy and combination therapy. First-line prescription of sulfonylurea was observed in 6.9% of patients aged 60-79 years and in 10.8% of patients aged ≥80 years. Patients starting with metformin showed fewer treatment modifications (10.4%) compared to patients initiating with sulfonylureas (35.2%). Newer ADs were utilized during treatment progression. Patients who initiated with sulfonylurea were approximately 70% more likely to discontinue treatment compared to those initiated on metformin. Oldest age group (≥80 years) was more likely to be non-persistent, and likelihood of non-persistence was highest in polymedicated patients. Patients changing therapy were more likely to be persistent. Our results show that treatment of T2D in Italy is consistent with clinical guidelines. Even if newer ADs were utilized during disease progression, they seem not to be preferred in patients with a higher comorbidity score, although these patients could benefit from this kind of treatment. Our study highlights patients' characteristics that might help identify those who would benefit from counselling from their health-care practitioner on better AD usage.
2型糖尿病患病率的稳步上升以及新型抗糖尿病药物(AD)的出现,使得这些药物的使用增加,且特定药物的使用模式发生了变化。这种治疗的复杂性源于为维持血糖控制而进行的连续治疗起始、换药和加药。本研究的目的是描述AD起始治疗、加药治疗和换药情况的使用模式,并衡量影响治疗持续性的因素。回顾性观察研究。数据从坎帕尼亚地区药物消费数据库中获取。研究人群为在2016年1月1日至12月31日期间接受至少一次AD处方的患者。我们将治疗换药或加药时间计算为中位数天数和四分位间距(IQR)。使用Kaplan-Meier方法估计持续性率。我们使用Cox回归模型估计随访1年期间不持续治疗的可能性。计算风险比和95%置信区间。在14679名患者中,86.9%开始采用单药治疗,13.1%开始采用联合治疗。单药治疗和联合治疗中最常见的初始治疗药物都是二甲双胍。在60-79岁的患者中,6.9%的患者一线处方为磺脲类药物,在80岁及以上的患者中这一比例为10.8%。与起始使用磺脲类药物的患者(35.2%)相比,起始使用二甲双胍的患者治疗调整较少(10.4%)。在治疗过程中使用了更新的AD。与起始使用二甲双胍的患者相比,起始使用磺脲类药物的患者停药可能性高出约70%。年龄最大的年龄组(≥80岁)更有可能不持续治疗,且在使用多种药物的患者中不持续治疗的可能性最高。更换治疗方案的患者更有可能持续治疗。我们的结果表明,意大利2型糖尿病的治疗符合临床指南。即使在疾病进展过程中使用了更新的AD,但在合并症评分较高的患者中,它们似乎并非首选,尽管这些患者可能从这类治疗中获益。我们的研究突出了患者的特征,这些特征可能有助于识别那些能从医疗保健从业者关于更好地使用AD的咨询中获益的患者。