Kumasi Centre for Collaborative Research in Tropical Medicine (KCCR), Kwame Nkrumah University of Science and Technology (KNUST), Kumasi, Ghana.
School of Biosciences and Medicine, University of Surrey, Guildford, United Kingdom.
PLoS Negl Trop Dis. 2019 Aug 26;13(8):e0007689. doi: 10.1371/journal.pntd.0007689. eCollection 2019 Aug.
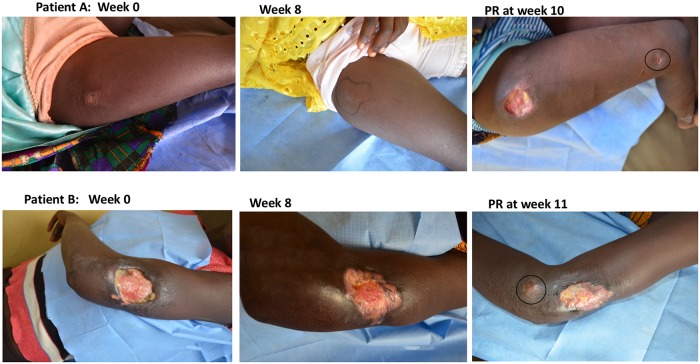
We investigated the relationship between bacterial load in Buruli ulcer (BU) lesions and the development of paradoxical reaction following initiation of antibiotic treatment.
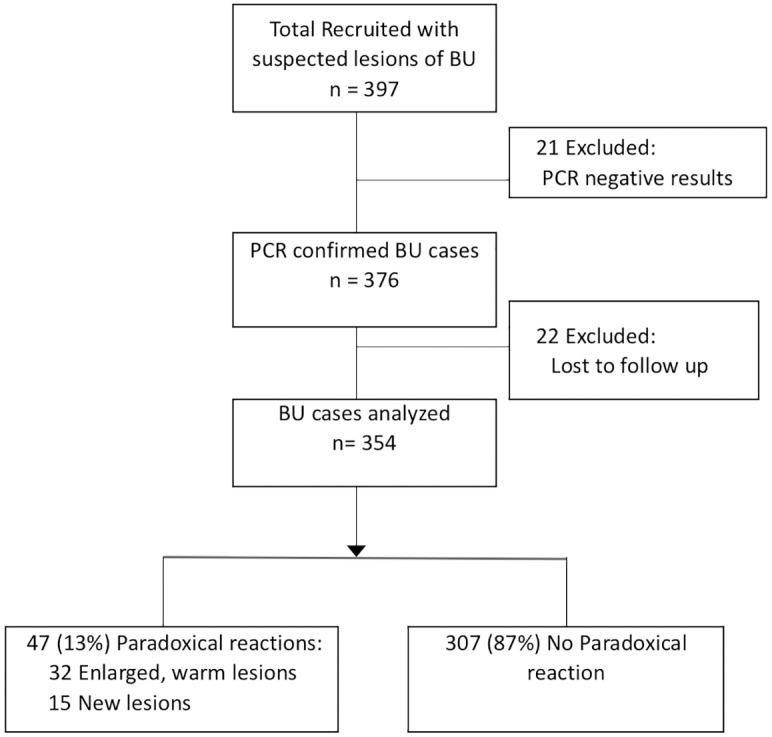
This was a longitudinal study involving BU patients from June 2013 to June 2017. Fine needle aspirates (FNA) and swab samples were obtained to establish the diagnosis of BU by PCR. Additional samples were obtained at baseline, during and after treatment (if the lesion had not healed) for microscopy, culture and combined 16S rRNA reverse transcriptase/ IS2404 qPCR assay. Patients were followed up at regular intervals until complete healing.
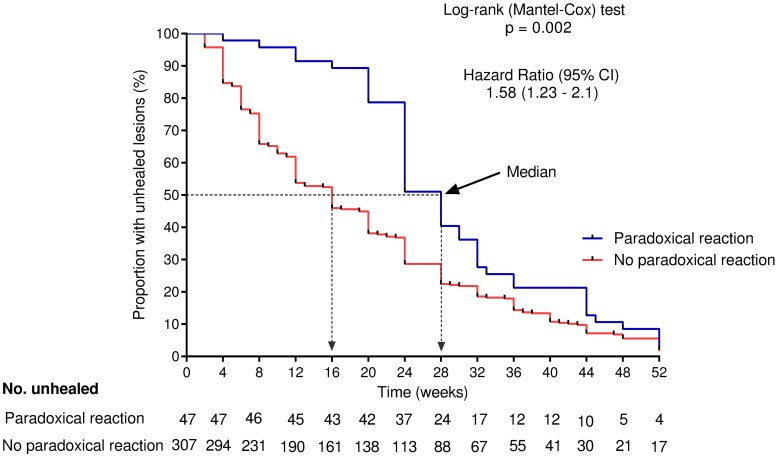
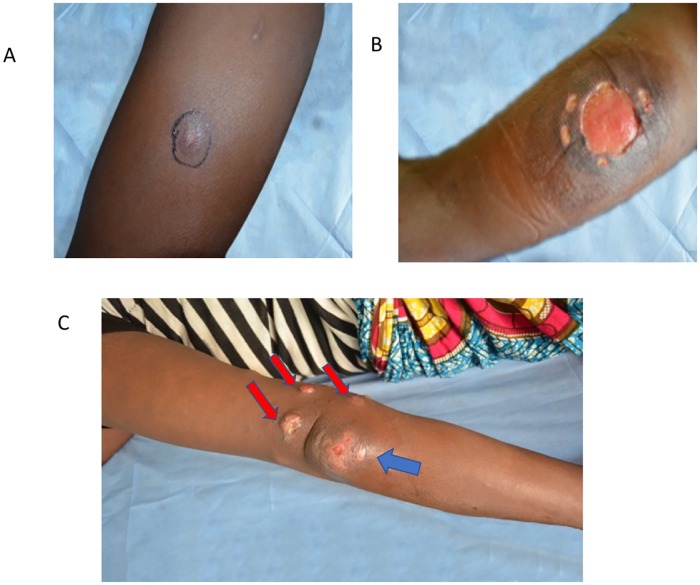
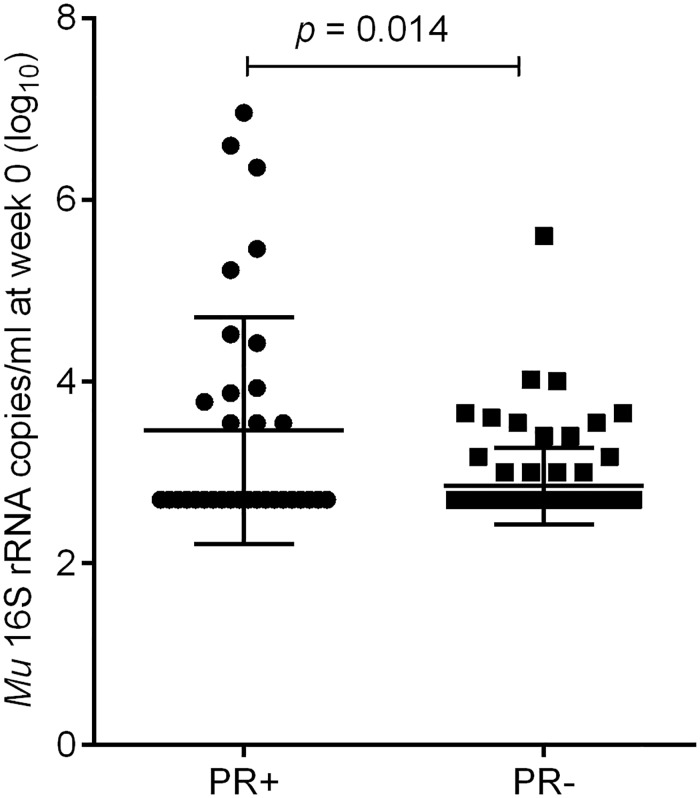
Forty-seven of 354 patients (13%) with PCR confirmed BU had a PR, occurring between 2 and 42 (median 6) weeks after treatment initiation. The bacterial load, the proportion of patients with positive M. ulcerans culture (15/34 (44%) vs 29/119 (24%), p = 0.025) and the proportion with positive microscopy results (19/31 (61%) vs 28/90 (31%), p = 0.003) before initiation of treatment were significantly higher in the PR compared to the no PR group. Plaques (OR 5.12; 95% CI 2.26-11.61; p<0.001), oedematous (OR 4.23; 95% CI 1.43-12.5; p = 0.009) and category II lesions (OR 2.26; 95% CI 1.14-4.48; p = 0.02) were strongly associated with the occurrence of PR. The median time to complete healing (28 vs 13 weeks, p <0.001) was significantly longer in the PR group.
Buruli ulcer patients who develop PR are characterized by high bacterial load in lesion samples taken at baseline and a higher rate of positive M. ulcerans culture. Occurrence of a PR was associated with delayed healing.
ClinicalTrials.gov NCT02153034.
我们研究了分枝杆菌负荷与抗结核药物治疗后出现矛盾反应之间的关系。
这是一项纵向研究,纳入了 2013 年 6 月至 2017 年 6 月的 354 例经聚合酶链反应(PCR)确诊的患者。通过细针抽吸(FNA)和拭子样本进行诊断。在基线、治疗期间(如果病变未愈合)和治疗后获得额外样本,用于显微镜检查、培养和联合 16S rRNA 逆转录酶/IS2404 qPCR 检测。患者定期随访至完全愈合。
47 例(13%)PCR 确诊的患者发生 PR,发生在治疗开始后 2 至 42 周(中位数 6 周)。PR 组的细菌负荷、分枝杆菌培养阳性率(15/34(44%)与 29/119(24%),p=0.025)和显微镜检查阳性率(19/31(61%)与 28/90(31%),p=0.003)在治疗开始前显著高于非 PR 组。斑块(OR 5.12;95%CI 2.26-11.61;p<0.001)、水肿(OR 4.23;95%CI 1.43-12.5;p=0.009)和 II 类病变(OR 2.26;95%CI 1.14-4.48;p=0.02)与 PR 的发生密切相关。PR 组完全愈合的中位时间(28 周与 13 周,p<0.001)显著延长。
发生 PR 的患者的病变样本中,基线时的细菌负荷较高,分枝杆菌培养阳性率也较高。PR 的发生与愈合延迟有关。
ClinicalTrials.gov NCT02153034。