School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana.
Department of Medicine, Komfo Anokye Teaching Hospital, Kumasi, Ghana.
BMC Infect Dis. 2021 Apr 8;21(1):331. doi: 10.1186/s12879-021-06009-7.
Previous studies have reported that presence and severity of Buruli ulcer (BU) may reflect the underlying immunosuppression in HIV infected individuals by causing increased incidence of multiple, larger and ulcerated lesions. We report cases of BU-HIV coinfection and the accompanying programmatic challenges encountered in central Ghana.
Patients with PCR confirmed BU in central Ghana who were HIV positive were identified and their BU01 forms were retrieved and reviewed in further detail. A combined 16S rRNA reverse transcriptase / IS2404 qPCR assay was used to assess the Mycobacterium ulcerans load. The characteristics of coinfected patients (BUHIV) were compared with a group of matched controls.
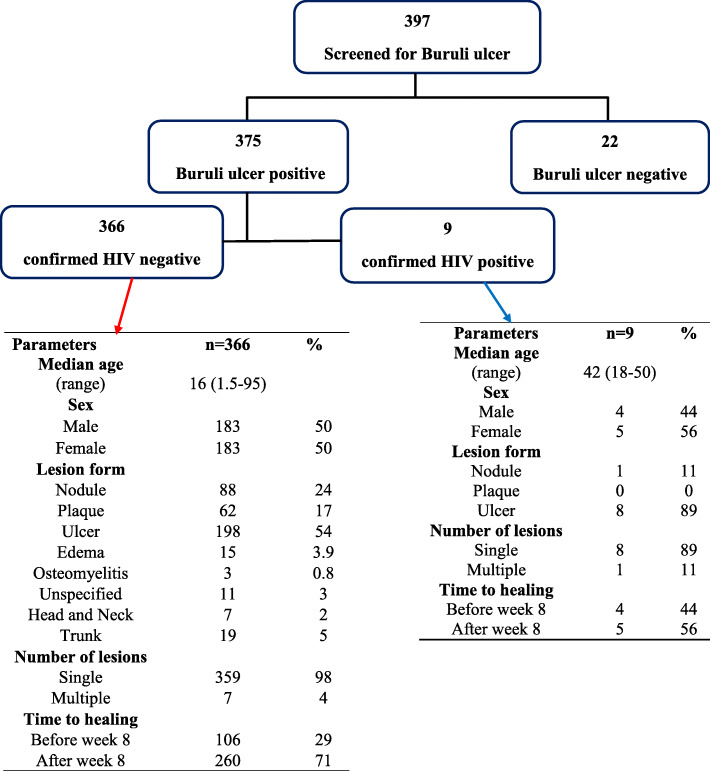
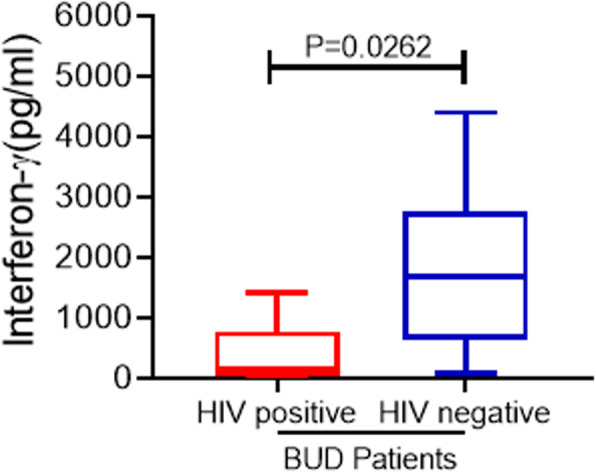
The prevalence of HIV in this BU cohort was 2.4% (compared to national HIV prevalence of 1.7%). Eight of 9 BUHIV patients had a single lesion and ulcers were the most common lesion type. The lesions presented were predominantly category II (5/9) followed by category I lesions. The median (IQR) time to healing was 14 (8-28) weeks in the BUHIV compared to 28 (12-33) weeks in the control BUHIV group (p = 0.360). Only one BUHIV developed a paradoxical reaction at week 16 but the lesion healed completely at week 20. The median bacterial load (16SrRNA) of BUHIV patients was 750 copies /ml (95% CI 0-398,000) versus 500 copies/ml (95% CI 0-126,855,500) in BUHIV group. Similarly, the median count using the IS2404 assay was 500 copies/ml (95% CI 0-500) for BUHIV patients versus 500 copies/ml (95% CI 500-31,000) for BUHIV patients. BUHIV patients mounted a significantly higher interferon-γ response compared to the BUHIV co-infected patients with respective median (range) responses of [1687(81.11-4399) pg/ml] versus [137.5(4.436-1406) pg/ml, p = 0.03]. There were challenges with the integration of HIV and BU care in this cohort.
The prevalence of HIV in the BU+ infected population was not significantly increased when compared to the prevalence of HIV in the general population. There was no clear relationship between BU lesion severity and HIV viral load or CD4 counts. Efforts should be made to encourage the integration of care of patients with BU-HIV coinfection.
先前的研究报告称,布路里溃疡(BU)的存在和严重程度可能反映了 HIV 感染者的潜在免疫抑制,导致多发性、更大和溃疡性病变的发病率增加。我们报告了加纳中部 BU-HIV 合并感染病例以及伴随的方案挑战。
在加纳中部,通过聚合酶链反应(PCR)确诊的 BU 患者中,确定 HIV 阳性患者,并进一步详细检索和审查其 BU01 表格。采用 16S rRNA 逆转录酶/IS2404 qPCR 联合检测评估溃疡分枝杆菌负荷。将合并感染患者(BUHIV)的特征与一组匹配的对照组进行比较。
该 BU 队列中 HIV 的流行率为 2.4%(而全国 HIV 的流行率为 1.7%)。9 例 BUHIV 患者中有 8 例有单个病变,溃疡是最常见的病变类型。病变主要为 II 类(5/9),其次是 I 类病变。BUHIV 组的愈合中位数(IQR)为 14 周(8-28 周),而对照组 BUHIV 组为 28 周(12-33 周)(p=0.360)。只有 1 例 BUHIV 在第 16 周出现矛盾反应,但第 20 周完全愈合。BUHIV 患者的细菌负荷中位数(16SrRNA)为 750 拷贝/ml(95%CI 0-398,000),而 BUHIV 组为 500 拷贝/ml(95%CI 0-126,855,500)。同样,使用 IS2404 检测的中位数计数为 500 拷贝/ml(95%CI 0-500)BUHIV 患者,而 BUHIV 患者为 500 拷贝/ml(95%CI 500-31,000)。与 BUHIV 患者相比,BUHIV 患者的干扰素-γ反应明显更高,中位数(范围)反应分别为[1687(81.11-4399)pg/ml]和[137.5(4.436-1406)pg/ml,p=0.03]。在该队列中,HIV 和 BU 护理的整合存在挑战。
与普通人群的 HIV 流行率相比,BU+感染人群中 HIV 的流行率没有显著增加。BU 病变严重程度与 HIV 病毒载量或 CD4 计数之间没有明确关系。应努力鼓励整合 BU-HIV 合并感染患者的护理。