Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Chronic Diseases and Ageing, Division of Mental and Physical Health, Norwegian Institute of Public Health, Oslo, Norway.
PLoS One. 2019 Aug 26;14(8):e0221500. doi: 10.1371/journal.pone.0221500. eCollection 2019.
To compare effectiveness and safety of warfarin and the direct oral anticoagulants (DOAC) dabigatran, rivaroxaban and apixaban in non-valvular atrial fibrillation in routine care.
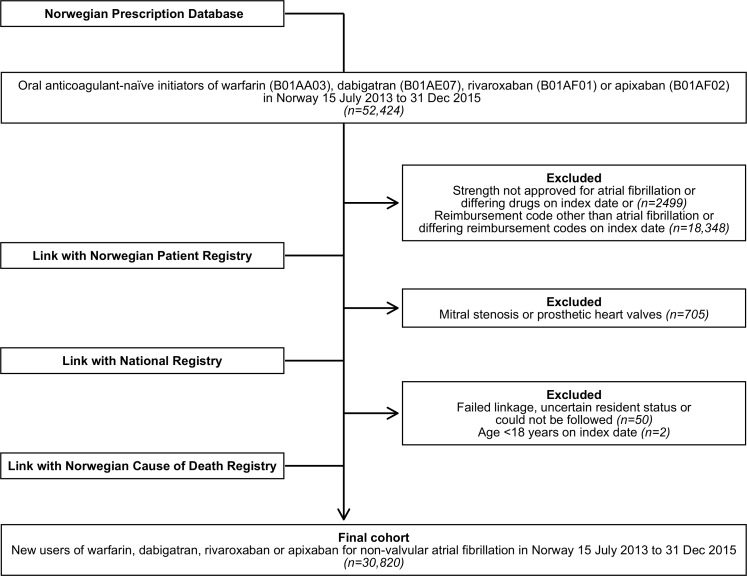
From nationwide registries, we identified treatment-naïve patients initiating warfarin, dabigatran, rivaroxaban or apixaban for non-valvular atrial fibrillation from July 2013 to December 2015 in Norway. We assessed prescription duration using reverse waiting time distribution. Adjusting for confounding in a Cox proportional hazards model, we estimated one-year risks for ischemic stroke, transient ischemic attack (TIA) or systemic embolism, major or clinically relevant non-major bleeding; intracranial; gastrointestinal; and other bleeding. We censored at switch of treatment or 365 days of follow-up.
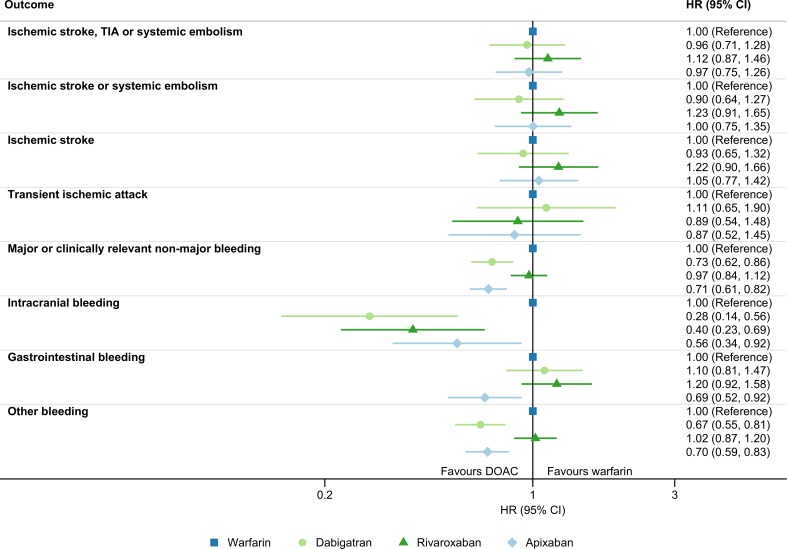
We included 30,820 treatment-naïve patients. Compared to warfarin, the adjusted hazard ratios (HR) for ischemic stroke, TIA or systemic embolism were 0.96 (95% CI 0.71-1.28) for dabigatran, 1.12 (95% CI 0.87-1.45) for rivaroxaban and 0.97 (95% CI 0.75-1.26) for apixaban. Corresponding hazard ratios for major or clinically relevant non-major bleeding were 0.73 (95% CI 0.62-0.86) for dabigatran, 0.97 (95% CI 0.84-1.12) for rivaroxaban and 0.71 (95% CI 0.62-0.82) for apixaban. Statistically significant differences of other safety outcomes compared to warfarin were fewer intracranial bleedings with dabigatran (HR 0.28, 95% CI 0.14-0.56), rivaroxaban (HR 0.40, 95% CI 0.23-0.69) and apixaban (HR 0.56, 95% CI 0.34-0.92); fewer gastrointestinal bleedings with apixaban (HR 0.70, 95% CI 0.52-0.93); and fewer other bleedings with dabigatran (HR 0.67, 95% CI 0.55-0.81) and apixaban (HR 0.70, 95% CI 0.59-0.83).
After 1 year follow-up in treatment-naïve patients initiating oral anticoagulation for non-valvular atrial fibrillation, all DOACs were similarly effective as warfarin in prevention of ischemic stroke, TIA or systemic embolism. Safety from bleedings was similar or better, including fewer intracranial bleedings with all direct oral anticoagulants, fewer gastrointestinal bleedings with apixaban and fewer other bleedings with dabigatran and apixaban.
比较非瓣膜性心房颤动患者在常规治疗中使用华法林和直接口服抗凝剂(DOAC)达比加群、利伐沙班和阿哌沙班的疗效和安全性。
从全国性登记处中,我们确定了 2013 年 7 月至 2015 年 12 月挪威治疗初治患者开始使用华法林、达比加群、利伐沙班或阿哌沙班治疗非瓣膜性心房颤动。我们使用反向等待时间分布评估处方持续时间。通过 Cox 比例风险模型进行混杂因素调整,我们估计了缺血性卒中、短暂性脑缺血发作(TIA)或全身性栓塞、大出血或临床相关非大出血;颅内;胃肠道;以及其他出血的一年风险。我们在治疗转换或 365 天随访时进行了删失。
我们纳入了 30820 名治疗初治患者。与华法林相比,达比加群的缺血性卒中、TIA 或全身性栓塞调整后的风险比(HR)为 0.96(95%CI 0.71-1.28),利伐沙班为 1.12(95%CI 0.87-1.45),阿哌沙班为 0.97(95%CI 0.75-1.26)。大出血或临床相关非大出血的相应风险比为达比加群 0.73(95%CI 0.62-0.86),利伐沙班 0.97(95%CI 0.84-1.12),阿哌沙班 0.71(95%CI 0.62-0.82)。与华法林相比,其他安全性结局的统计学显著差异为达比加群的颅内出血更少(HR 0.28,95%CI 0.14-0.56),利伐沙班(HR 0.40,95%CI 0.23-0.69)和阿哌沙班(HR 0.56,95%CI 0.34-0.92);阿哌沙班的胃肠道出血更少(HR 0.70,95%CI 0.52-0.93);达比加群和阿哌沙班的其他出血更少(HR 0.67,95%CI 0.55-0.81)和(HR 0.70,95%CI 0.59-0.83)。
在治疗初治非瓣膜性心房颤动患者开始口服抗凝治疗的 1 年后,所有 DOAC 与华法林在预防缺血性卒中、TIA 或全身性栓塞方面同样有效。出血安全性相似或更好,包括所有直接口服抗凝剂的颅内出血更少,阿哌沙班的胃肠道出血更少,达比加群和阿哌沙班的其他出血更少。