Dartmouth Hitchcock Medical Center, Lebanon, USA.
Geisel School of Medicine at Dartmouth, Hanover, USA.
BMC Pregnancy Childbirth. 2019 Aug 27;19(1):309. doi: 10.1186/s12884-019-2454-9.
Induction of labor occurs in greater than 22% of all pregnancies in the United States. Previous studies have shown that misoprostol is more effective for induction than oxytocin or dinoprostone alone. The World Health Organization recommends vaginal misoprostol 25mcg every 6 hours and the American Congress of Obstetricians and Gynecologists recommends 25mcg vaginal misoprostol every three to 6 hours. Although route of administration and dosage of misoprostol has been extensively studied, little is known about the optimal dosing interval of vaginal misoprostol.
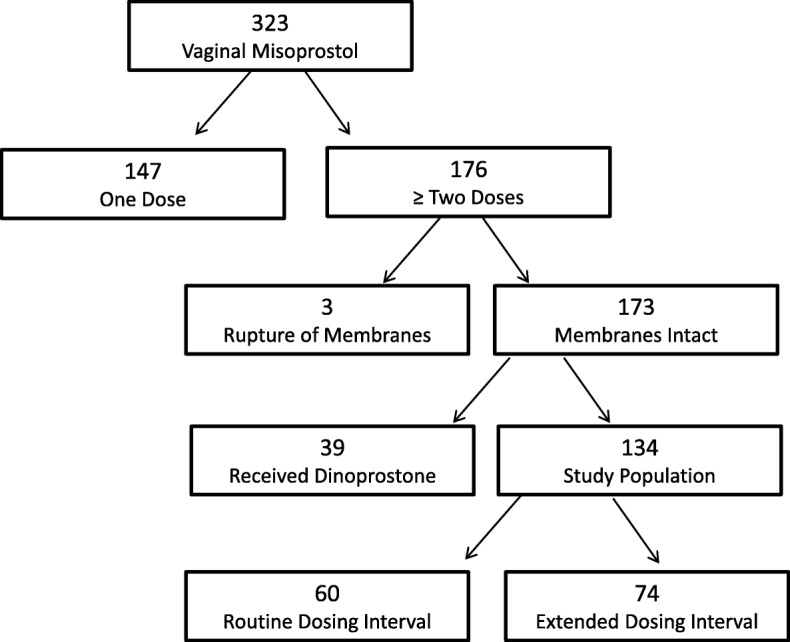
The primary objective of this study is to determine the effect of delayed vaginal misoprostol dosing, defined as any interval longer than 4.5 h, on time to vaginal delivery. Our hypothesis is that the routine dosing interval of 4 hours shortens times to vaginal delivery compared to delayed dosing, even when adjusted for the time of delay. Secondary objectives include the effect of delayed vaginal misoprostol dosing on cesarean section rate, operative vaginal delivery rate, maternal outcomes, and neonatal outcomes. We conducted a retrospective chart review of 323 inductions of labor at one academic institution. The primary outcome was the proportion of patients who achieved a vaginal delivery within 24 h. The group who received all doses of misoprostol within a 4.5 h dosing window (Routine Dosing Interval Group) was compared with the group who had any dosing deviation (Delayed Dosing Interval Group).
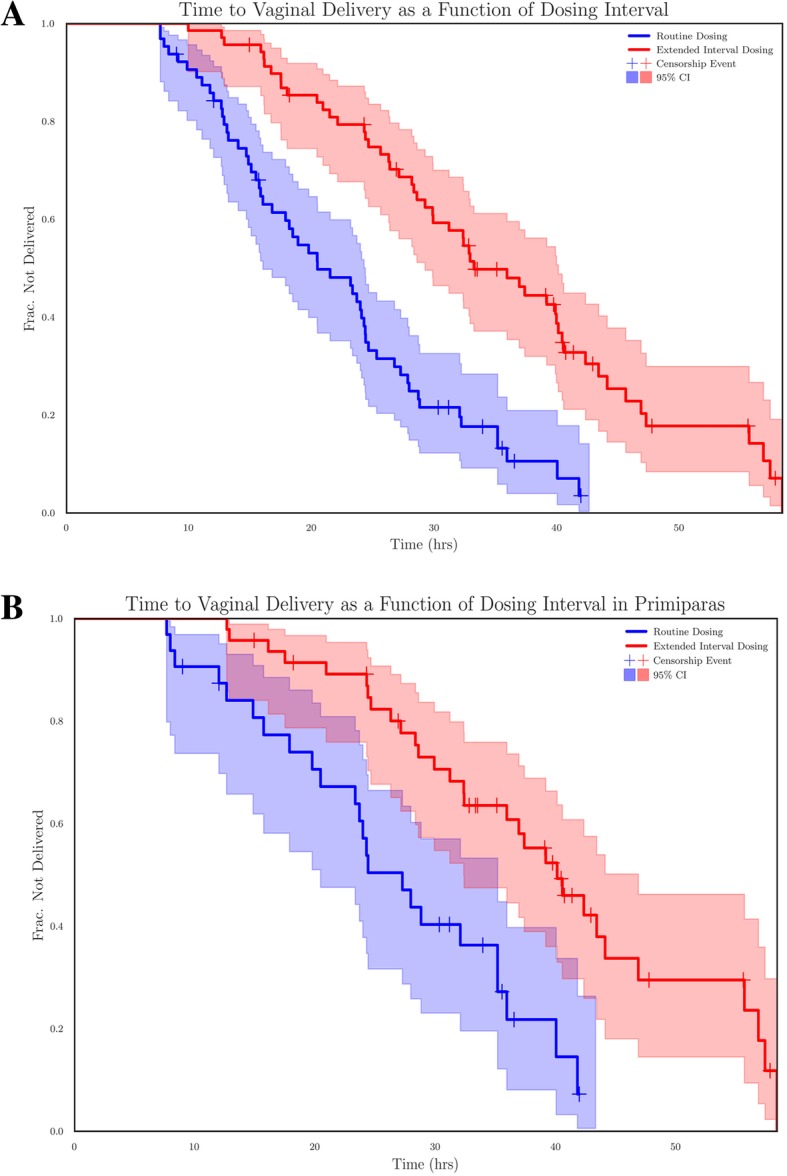
Of 133 included patients, 64 subjects received routine interval dosing and 69 subjects received delayed interval dosing. The vaginal delivery rates within 24 h were 56% (36/64) and 20% (14/69), respectively (P < 10). Spontaneous vaginal delivery rates were 86% (55/64) vs. 75% (52/69), respectively (P = .13). Kaplan Meier curves demonstrated statistically significant difference in time to vaginal delivery between groups, with a Cox Proportional Hazard ratio for routine dosing interval of 1.73 (P < 10) unadjusted and 1.34 (P = .01) when adjusted for dosing delay.
This retrospective study demonstrates a significant increase in delay-adjusted time to vaginal delivery when doses of vaginal misoprostol are delayed past 4.5 h.
在美国,超过 22%的孕妇需要引产。先前的研究表明,米索前列醇在引产方面比催产素或地诺前列酮更有效。世界卫生组织建议每 6 小时阴道内使用 25mcg 米索前列醇,美国妇产科医师学会建议每 3 至 6 小时阴道内使用 25mcg 米索前列醇。虽然米索前列醇的给药途径和剂量已经得到了广泛的研究,但对于阴道内米索前列醇的最佳给药间隔时间知之甚少。
本研究的主要目的是确定阴道内米索前列醇延迟给药(定义为任何超过 4.5 小时的间隔)对阴道分娩时间的影响。我们的假设是,与延迟给药相比,常规 4 小时给药间隔可以缩短阴道分娩时间,即使在调整了延迟时间的情况下也是如此。次要目标包括延迟阴道内米索前列醇给药对剖宫产率、阴道分娩率、产妇结局和新生儿结局的影响。我们对一家学术机构的 323 例引产进行了回顾性图表审查。主要结局是 24 小时内实现阴道分娩的患者比例。接受 4.5 小时给药窗口内所有米索前列醇剂量的患者(常规给药间隔组)与接受任何给药偏差的患者(延迟给药间隔组)进行比较。
在纳入的 133 例患者中,64 例接受常规间隔给药,69 例接受延迟间隔给药。24 小时内阴道分娩率分别为 56%(36/64)和 20%(14/69)(P<0.01)。自发性阴道分娩率分别为 86%(55/64)和 75%(52/69)(P=0.13)。Kaplan-Meier 曲线显示两组间阴道分娩时间存在统计学显著差异,常规给药间隔的 Cox 比例风险比为 1.73(P<0.01),未调整时为 1.34(P=0.01),调整给药延迟时为 1.34(P=0.01)。
这项回顾性研究表明,当阴道内米索前列醇的剂量延迟超过 4.5 小时时,调整后的阴道分娩时间显著延长。