Wang Kun, Gong Meihua, Xie Songpu, Zhang Meng, Zheng Huabo, Zhao XiaoFang, Liu Chengyun
1Department of Geriatrics, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022 China.
Department of Clinical Laboratory, The Third People Hospital of Jimo, Jimo, 266000 Shandong China.
EPMA J. 2019 Aug 6;10(3):227-237. doi: 10.1007/s13167-019-00181-2. eCollection 2019 Sep.
To develop a precise personalized type 2 diabetes mellitus (T2DM) prediction model by cost-effective and readily available parameters in a Central China population.
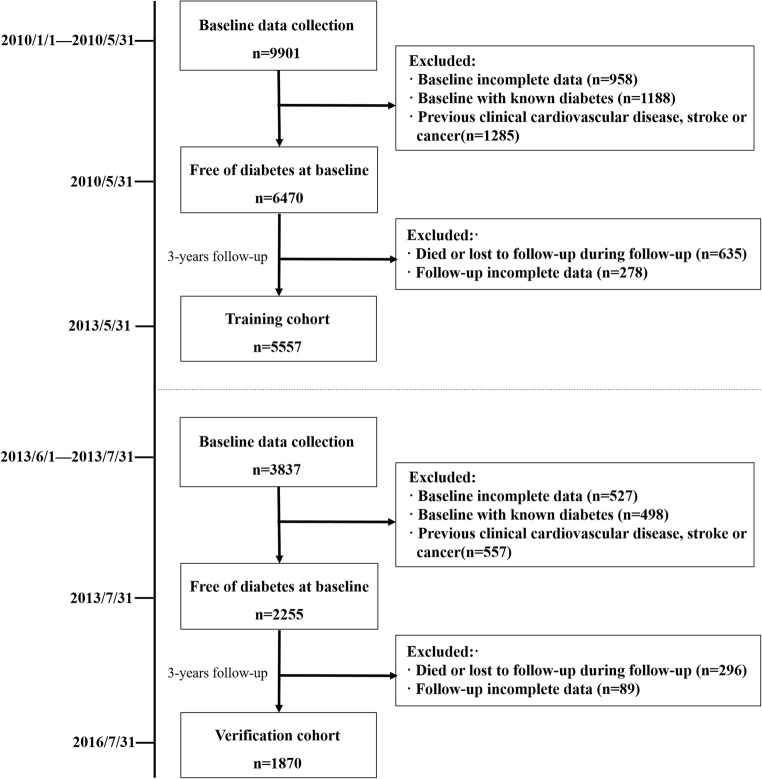
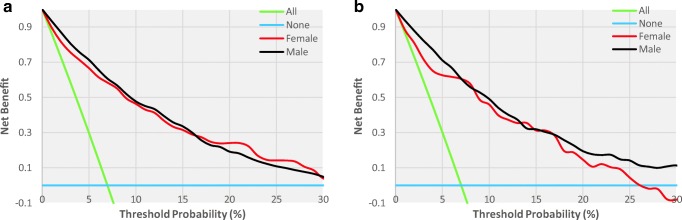
A 3-year cohort study was performed on 5557 nondiabetic individuals who underwent annual physical examination as the training cohort, and a subsequent validation cohort of 1870 individuals was conducted using the same procedures. Multiple logistic regression analysis was performed, and a simple nomogram was constructed via the stepwise method. Receiver operating characteristic (ROC) curve and decision curve analyses were performed by 500 bootstrap resamplings to assess the determination and clinical value of the nomogram, respectively. We also estimated the optimal cutoff values of each risk factor for T2DM prediction.
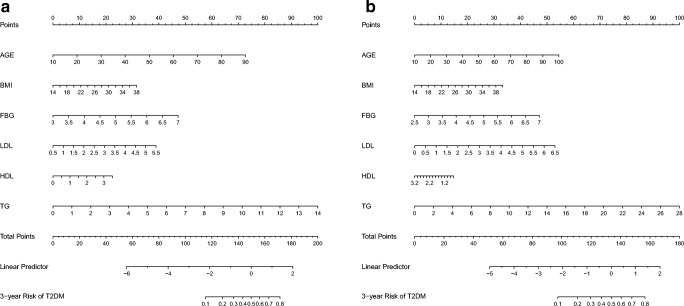
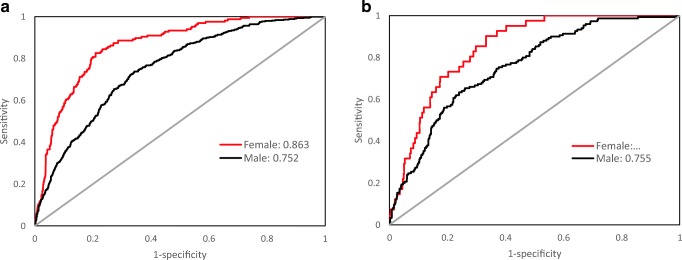
The 3-year cumulative incidence of T2DM was 10.71%. We developed simple nomograms that predict the risk of T2DM for females and males by using the parameters of age, BMI, fasting blood glucose (FBG), low-density lipoprotein cholesterol (LDLc), high-density lipoprotein cholesterol (HDLc), and triglycerides (TG). In the training cohort, the area under the ROC curve (AUC) showed statistical accuracy (AUC = 0.863 for female, AUC = 0.751 for male), and similar results were shown in the subsequent validation cohort (AUC = 0.847 for female, AUC = 0.755 for male). Decision curve analysis demonstrated the clinical value of this nomogram. To optimally predict the risk of T2DM, the cutoff values of age, BMI, FBG, systolic blood pressure, diastolic blood pressure, total cholesterol, LDLc, HDLc, and TG were 47.5 and 46.5 years, 22.9 and 23.7 kg/m, 5.1 and 5.4 mmol/L, 118 and 123 mmHg, 71 and 85 mmHg, 5.06 and 4.94 mmol/L, 2.63 and 2.54 mmol/L, 1.53 and 1.34 mmol/L, and 1.07 and 1.65 mmol/L for females and males, respectively.
Our nomogram can be used as a simple, plausible, affordable, and widely implementable tool to predict a personalized risk of T2DM for Central Chinese residents. The successful identification of at-risk individuals and intervention at an early stage can provide advanced strategies from a predictive, preventive, and personalized medicine perspective.
利用华中地区人群中经济高效且易于获得的参数,开发一种精确的个性化2型糖尿病(T2DM)预测模型。
对5557名接受年度体检的非糖尿病个体进行了为期3年的队列研究作为训练队列,并对1870名个体采用相同程序进行了后续验证队列研究。进行了多因素逻辑回归分析,并通过逐步法构建了一个简单的列线图。通过500次自抽样重采样进行受试者操作特征(ROC)曲线和决策曲线分析,分别评估列线图的判别能力和临床价值。我们还估计了每个风险因素用于T2DM预测的最佳截断值。
T2DM的3年累积发病率为10.71%。我们通过使用年龄、体重指数(BMI)、空腹血糖(FBG)、低密度脂蛋白胆固醇(LDLc)、高密度脂蛋白胆固醇(HDLc)和甘油三酯(TG)等参数,开发了可预测女性和男性T2DM风险的简单列线图。在训练队列中,ROC曲线下面积(AUC)显示出统计学准确性(女性AUC = 0.863,男性AUC = 0.751),在后续验证队列中也得到了类似结果(女性AUC = 0.847,男性AUC = O.755)。决策曲线分析证明了该列线图的临床价值。为了最佳地预测T2DM风险,女性和男性的年龄、BMI、FBG、收缩压、舒张压、总胆固醇、LDLc、HDLc和TG的截断值分别为47.5和46.5岁、22.9和23.7kg/m²、5.1和5.4mmol/L、118和123mmHg、71和85mmHg、5.06和4.94mmol/L、2.63和2.54mmol/L、1.53和1.34mmol/L以及1.07和1.65mmol/L。
我们的列线图可作为一种简单、合理、经济且可广泛应用的工具,用于预测华中地区居民个性化的T2DM风险。成功识别高危个体并在早期进行干预,可从预测、预防和个性化医学角度提供先进策略。