Division of Health Policy and Management, School of Public Health, University of Minnesota, Minneapolis.
Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
JAMA Netw Open. 2019 Aug 2;2(8):e1910373. doi: 10.1001/jamanetworkopen.2019.10373.
Time pressure to provide a quick fix is commonly cited as a reason why opioids are frequently prescribed in the United States, but there is little evidence of an association between appointment timing and clinical decision-making. As the workday progresses and appointments run behind schedule, physicians may be more likely to prescribe opioids.
To estimate whether characteristics of appointment timing are associated with clinical decision-making about pain treatment.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study of physician behavior used data from electronic health record systems in primary care offices in the United States to analyze primary care appointments occurring in 2017 for patients with a new painful condition who had not received an opioid prescription within the past year.
The association between treatment decisions and 2 dimensions of appointment timing (order of appointment occurrence and delay relative to scheduled start time) were assessed. The rates of opioid prescribing were measured and compared with rates of nonopioid pain medication (ie, nonsteroidal anti-inflammatory drugs) prescribing and referral to physical therapy. All rates were estimated within the same physician using physician fixed effects, adjusting for patient, appointment, and seasonal characteristics.
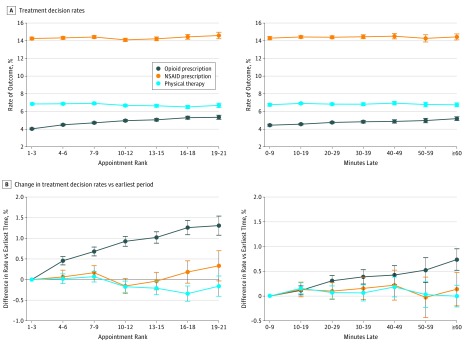
Among 678 319 primary care appointments (642 262 patients; 392 422 [61.1%] women) with 5603 primary care physicians, the likelihood that an appointment resulted in an opioid prescription increased by 33% as the workday progressed (1st to 3rd appointment, 4.0% [95% CI, 3.9%-4.1%] vs 19th to 21st appointment, 5.3% [95% CI. 5.1%-5.6%]; P < .001) and by 17% as appointments ran behind schedule (0-9 minutes late, 4.4% [95% CI, 4.3%-4.6%] vs ≥60 minutes late, 5.2% [95% CI, 5.0%-5.4%]; P < .001). Prescribing of nonsteroidal anti-inflammatory drugs and referral to physical therapy did not display similar patterns.
These findings suggest that, even within an individual physician's schedule, clinical decision-making for opioid prescribing varies by the timing and lateness of appointments.
在美国,提供快速解决方案的时间压力通常被认为是经常开处阿片类药物的原因,但预约时间与临床决策之间的关联几乎没有证据。随着工作日的推进和预约滞后,医生可能更倾向于开阿片类药物。
评估预约时间特征是否与疼痛治疗的临床决策相关。
设计、地点和参与者:这是一项在美国初级保健诊所电子健康记录系统中进行的医师行为横断面研究,分析了 2017 年新出现疼痛症状且过去一年未开具阿片类药物处方的患者的初级保健预约情况。
评估了治疗决策与预约时间的 2 个维度(预约发生的顺序和相对于预定开始时间的延迟)之间的关联。测量了开处阿片类药物的比率,并与开处非阿片类止痛药(即非甾体抗炎药)和转介物理治疗的比率进行比较。使用医师固定效应,在调整患者、预约和季节性特征后,在同一位医师内对所有比率进行了估计。
在 678319 次初级保健预约(642262 名患者;392422 名[61.1%]女性)中,共有 5603 名初级保健医生,随着工作日的推进,预约结果开出阿片类药物处方的可能性增加了 33%(第 1 至第 3 次预约为 4.0%[95%CI,3.9%-4.1%],第 19 至第 21 次预约为 5.3%[95%CI,5.1%-5.6%];P<.001),预约滞后的可能性增加了 17%(0-9 分钟延迟为 4.4%[95%CI,4.3%-4.6%],≥60 分钟延迟为 5.2%[95%CI,5.0%-5.4%];P<.001)。非甾体抗炎药的处方和物理治疗的转介并没有显示出类似的模式。
这些发现表明,即使在单个医生的日程安排内,阿片类药物处方的临床决策也会因预约时间和滞后时间而有所不同。