K C Shiva Raj, K C Geetika, Gyawali Purnima, Singh Manisha, Sijapati Milesh Jung
Department of Pathology, KIST Medical College, Imadol, Lalitpur, Nepal.
Department of Pathology and Laboratory Medicine, Patan Academy of Health Sciences, Lagankhel, Lalitpur, Nepal.
J Med Case Rep. 2019 Sep 1;13(1):276. doi: 10.1186/s13256-019-2198-1.
Leprosy is a disease that was declared eliminated in 2010 from Nepal; however, new cases are diagnosed every year. The difficulty arises when the presentation of the patient is unusual.
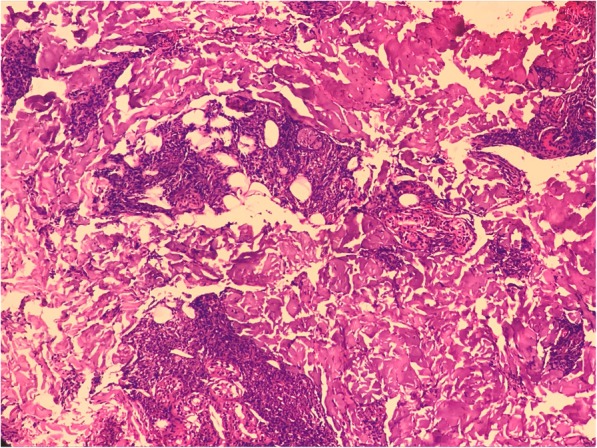
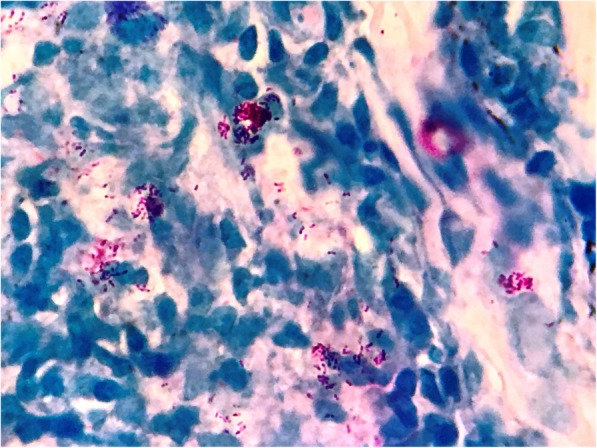
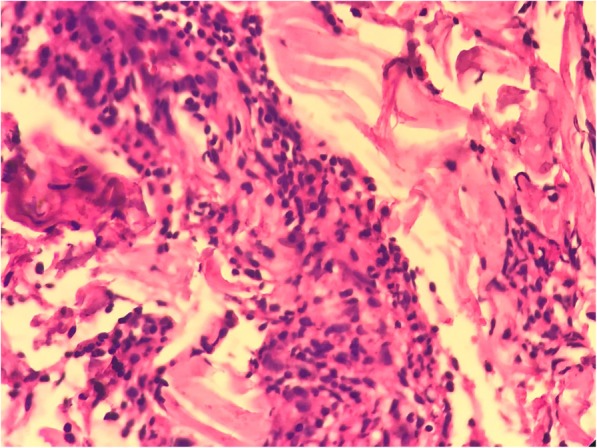
In this case report we present a case of a 22-year-old Tamang man, from the Terai region of Nepal, with a clinical presentation of fever, malaise, and arthralgia for the past 2 weeks with hepatosplenomegaly and bilateral cervical, axillary, and inguinal lymphadenopathy. Features of chronic inflammation with elevated erythrocyte sedimentation rate of 90 mm/hour and liver enzymes were noted. With no specific investigative findings, a diagnosis of Still's disease was made and he was given prednisolone. On tapering the medication, after 2 weeks, the lymphadenopathy and fever reappeared. On biopsy of a lymph node, diagnosis of possible tuberculosis was made. On that basis anti-tuberculosis treatment category I was started. During his hospital stay, our patient developed nodular skin rashes on his shoulder, back, and face. The biopsy of a skin lesion showed erythema nodosum leprosum and he was diagnosed as having lepromatous leprosy with erythema nodosum leprosum; he was treated with anti-leprosy medication.
An unusual presentations of leprosy may delay its prompt diagnosis and treatment; thus, increasing morbidity and mortality. Although leprosy has been declared eliminated, it should not be forgotten and physicians should have it in mind to make it a differential diagnosis whenever relevant.
麻风病是一种在2010年宣布已在尼泊尔消除的疾病;然而,每年仍有新病例被诊断出来。当患者的临床表现不寻常时,诊断就会出现困难。
在本病例报告中,我们呈现了一名来自尼泊尔特莱地区的22岁塔芒族男子的病例,他在过去两周出现发热、不适和关节痛的临床表现,伴有肝脾肿大以及双侧颈部、腋窝和腹股沟淋巴结肿大。注意到有慢性炎症的特征,红细胞沉降率升高至90毫米/小时,肝功能酶也异常。由于没有特异性的检查结果,诊断为斯蒂尔病,并给予泼尼松龙治疗。在用药逐渐减量2周后,淋巴结肿大和发热再次出现。对一个淋巴结进行活检后,诊断为可能的结核病。在此基础上开始了I类抗结核治疗。在他住院期间,我们的患者在肩部、背部和面部出现了结节性皮疹。对一处皮肤病变进行活检显示为麻风结节性红斑,他被诊断为瘤型麻风伴麻风结节性红斑;随后接受了抗麻风病药物治疗。
麻风病不寻常的表现可能会延迟其及时诊断和治疗;从而增加发病率和死亡率。尽管麻风病已被宣布消除,但不应被遗忘,医生在相关情况下应将其作为鉴别诊断考虑在内。