The George Institute for Global Health, University of Oxford, Oxford, England.
Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Nuffield Orthopaedic Centre, Oxford, England.
JAMA Cardiol. 2019 Nov 1;4(11):1102-1111. doi: 10.1001/jamacardio.2019.3593.
Despite considerable improvements in heart failure care, mortality rates among patients in high-income countries have changed little since the early 2000s. Understanding the reasons underlying these trends may provide valuable clues for developing more targeted therapies and public health strategies.
To investigate mortality rates following a new diagnosis of heart failure and examine changes over time and by cause of death and important patient features.
DESIGN, SETTING, AND PARTICIPANTS: This population-based retrospective cohort study analyzed anonymized electronic health records of individuals who received a new diagnosis of heart failure between January 2002 and December 2013 who were followed up until December 2014 from the Clinical Practice Research Datalink, which links information from primary care, secondary care, and the national death registry from a subset of the UK population. The data were analyzed from January 2018 to February 2019.
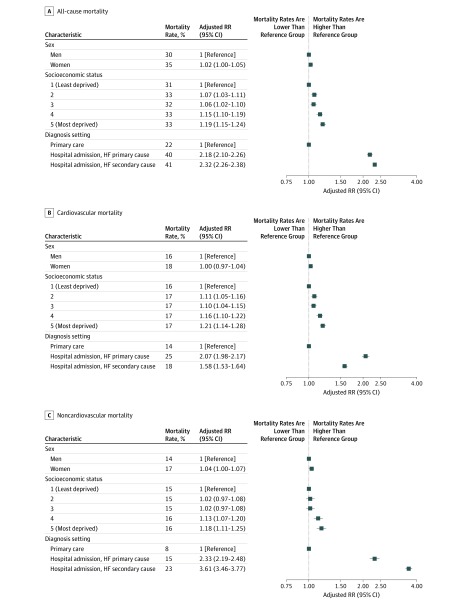
All-cause and cause-specific mortality rates at 1 year following diagnosis. Poisson regression models were used to calculate rate ratios (RRs) and 95% confidence intervals comparing 2013 with 2002, adjusting for age, sex, region, socioeconomic status, and 17 major comorbidities.
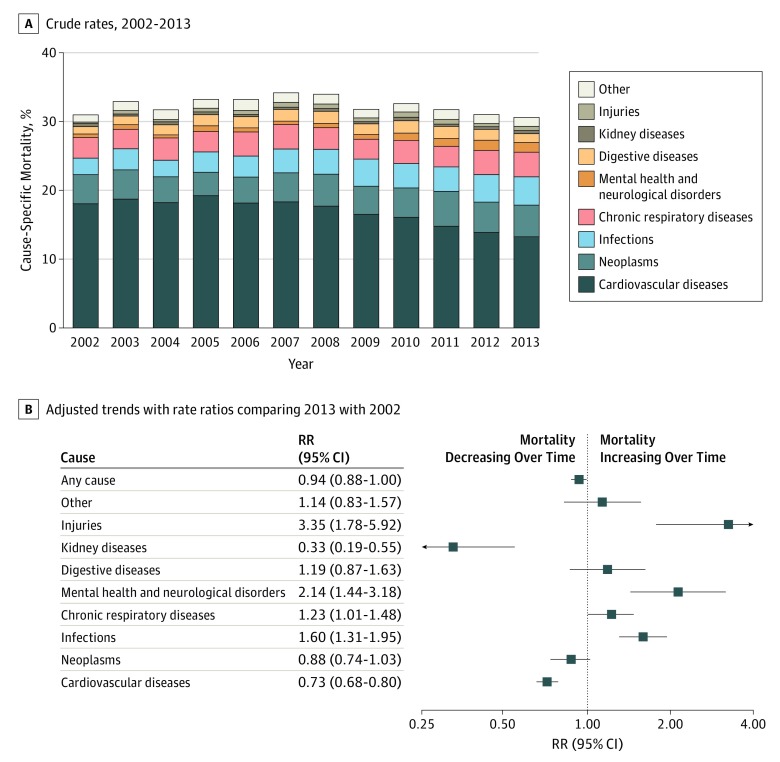
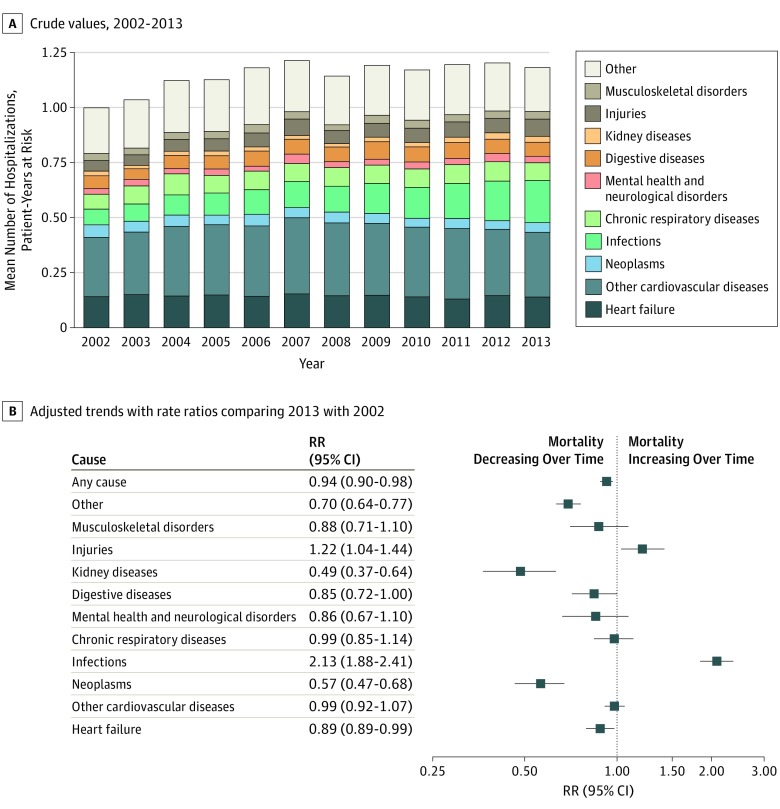
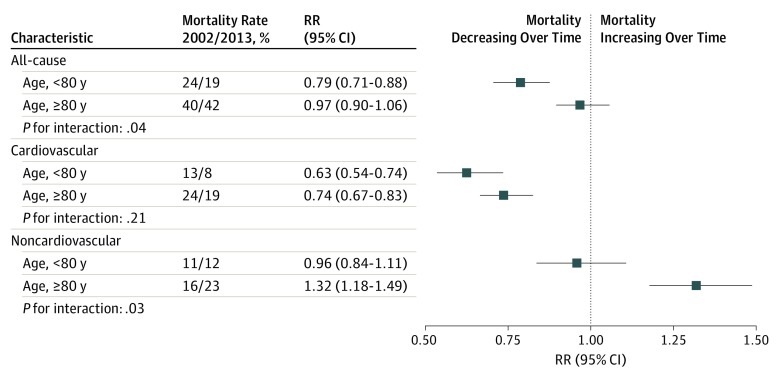
Of 86 833 participants, 42 581 (49%) were women, 51 215 (88%) were white, and the mean (SD) age was 76.6 (12.6) years. While all-cause mortality rates declined only modestly over time (RR comparing 2013 with 2002, 0.94; 95% CI, 0.88-1.00), underlying patterns presented explicit trends. A decline in cardiovascular mortality (RR, 0.73; 95% CI, 0.67-0.80) was offset by an increase in noncardiovascular deaths (RR, 1.22; 95% CI, 1.11-1.33). Subgroup analyses further showed that overall mortality rates declined among patients younger than 80 years (RR, 0.79; 95% CI, 0.71-0.88) but not among those older than 80 years (RR, 0.97; 95% CI, 0.90-1.06). After cardiovascular causes (898 [43%]), the major causes of death in 2013 were neoplasms (311 [15%]), respiratory conditions (243 [12%]), and infections (13%), the latter 2 explaining most of the observed increase in noncardiovascular mortality.
Among patients with a new heart failure diagnosis, considerable progress has been achieved in reducing mortality in young and middle-aged patients and cardiovascular mortality across all age groups. Improvements to overall mortality are hindered by high and increasing rates of noncardiovascular events. These findings challenge current research priorities and management strategies and call for a greater emphasis on associated comorbidities. Specifically, infection prevention presents as a major opportunity to improve prognosis.
尽管在心力衰竭治疗方面取得了相当大的进展,但自 21 世纪初以来,高收入国家患者的死亡率几乎没有变化。了解这些趋势背后的原因可能为开发更有针对性的治疗方法和公共卫生策略提供有价值的线索。
调查新诊断为心力衰竭患者的死亡率,并研究随时间的变化以及死因和重要患者特征的变化。
设计、设置和参与者:这项基于人群的回顾性队列研究分析了 2002 年 1 月至 2013 年 12 月期间新诊断为心力衰竭的患者的匿名电子健康记录,这些患者在临床实践研究数据链接(Clinical Practice Research Datalink)中进行了随访,该链接将来自英国部分人群的初级保健、二级保健和国家死亡登记处的信息联系起来。数据于 2018 年 1 月至 2019 年 2 月进行分析。
诊断后 1 年的全因和死因特异性死亡率。使用泊松回归模型计算 2013 年与 2002 年相比的比率比(RR)和 95%置信区间,调整年龄、性别、地区、社会经济状况和 17 种主要合并症。
在 86833 名参与者中,42581 名(49%)为女性,51215 名(88%)为白人,平均(SD)年龄为 76.6(12.6)岁。虽然全因死亡率随时间仅略有下降(2013 年与 2002 年相比的 RR,0.94;95%CI,0.88-1.00),但潜在模式呈现出明确的趋势。心血管死亡率下降(RR,0.73;95%CI,0.67-0.80)被非心血管死亡增加所抵消(RR,1.22;95%CI,1.11-1.33)。进一步的亚组分析表明,年龄小于 80 岁的患者的总体死亡率下降(RR,0.79;95%CI,0.71-0.88),但年龄大于 80 岁的患者的死亡率没有下降(RR,0.97;95%CI,0.90-1.06)。心血管原因(898[43%])后,2013 年的主要死因是肿瘤(311[15%])、呼吸状况(243[12%])和感染(13%),后两者解释了大部分观察到的非心血管死亡率增加。
在新诊断为心力衰竭的患者中,在降低年轻和中年患者的死亡率以及所有年龄段的心血管死亡率方面已经取得了相当大的进展。整体死亡率的提高受到非心血管事件发生率高且不断上升的阻碍。这些发现对当前的研究重点和管理策略提出了挑战,并呼吁更加重视相关合并症。具体来说,预防感染是改善预后的一个主要机会。