Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Medical Research Center, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China.
Department of Radiation Oncology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China.
J Appl Clin Med Phys. 2019 Sep;20(9):31-41. doi: 10.1002/acm2.12688. Epub 2019 Sep 4.
To investigate the fixed-jaw intensity-modulated radiotherapy (F-IMRT) and tangential partial volumetric modulated arc therapy (tP-VMAT) treatment plans for synchronous bilateral breast cancer (SBBC).
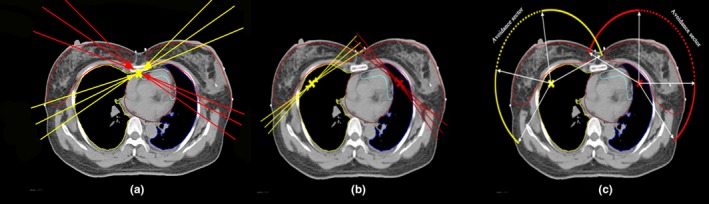
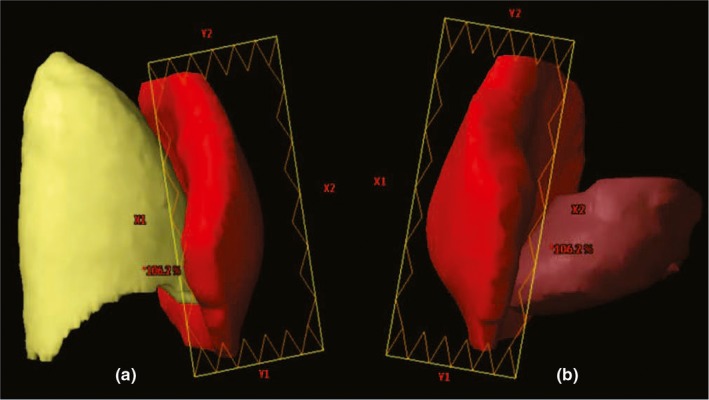
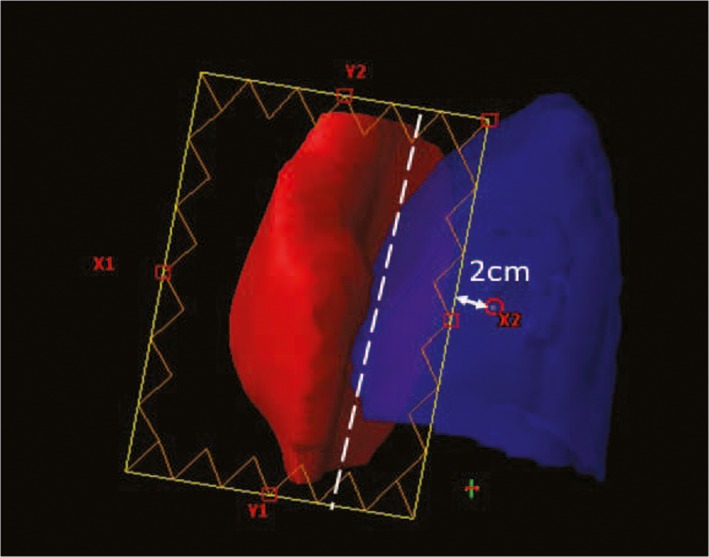
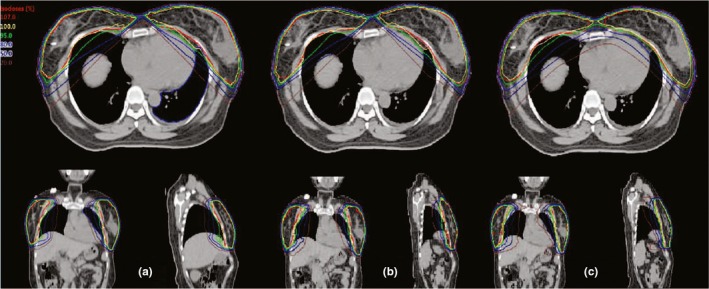
Twelve SBBC patients with pTis-2N0M0 stages who underwent whole-breast irradiation after breast-conserving surgery were planned with F-IMRT and tP-VMAT techniques prescribing 42.56 Gy (2.66 Gy*16f) to the breast. The F-IMRT used 8-12 jaw-fixed tangential fields with single (sF-IMRT) or two (F-IMRT) isocenters located under the sternum or in the center of the left and right planning target volumes (PTVs), and tP-VMAT used 4 tangential partial arcs with two isocenters located in the center of the left and right PTVs. Plan evaluation was based on dose-volume histogram (DVH) analysis. Dosimetric parameters were calculated to evaluate plan quality; total monitor units (MUs), and the gamma analysis for patient-specific quality assurance (QA) were also evaluated.
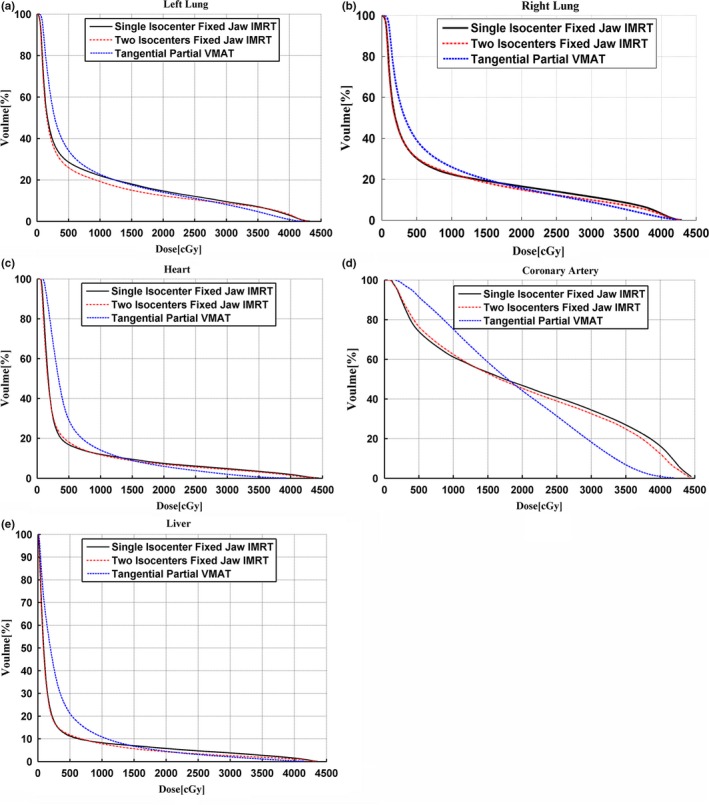
For PTVs, the three plans had similar D and conformity index (CI) values. F-IMRT showed a slightly better target coverage according to the V values and demonstrated an obvious reduction in V and D compared with the values observed for sF-IMRT and tP-VMAT. Compared with tP-VMAT, sF-IMRT was slightly better in terms of V , V and D . In addition, F-IMRT achieved the best homogeneity index (HI) values for PTVs. Concerning healthy tissue, tP-VMAT had an advantage in minimizing the high dose volume. The MUs of the tP-VMAT plan were decreased approximately 1.45 and 1 times compared with the sF-IMRT and F-IMRT plans, respectively, and all plans passed QA. For the lungs, heart and liver, F-IMRT achieved the smallest values in terms of D and showed a significant difference compared with tP-VMAT. Simultaneously, sF-IMRT was also superior to tP-VMAT. For the coronary artery, tP-VMAT achieved the lowest D , while the value for F-IMRT was 2.24% lower compared with sF-IMRT. For all organs at risk (OARs), tP-VMAT was superior at the high dose level. In contrast, sF-IMRT and F-IMRT were obviously superior at the low dose level. The sF-IMRT and F-IMRT plans showed consistent trends.
All treatment plans for the provided techniques were of high quality and feasible for SBBC patients. However, we recommend F-IMRT with a single isocenter as a priority technique because of the tremendous advantage of local hot spot control in PTVs and the reduced dose to OARs at low dose levels. When the irradiated dose to the lungs and heart exceed the clinical restriction, two isocenter F-IMRT can be used to maximize OAR sparing. Additionally, tP-VMAT can be adopted for improving cold spots in PTVs or high-dose exposure to normal tissue when the interval between PTVs is narrow.
研究固定 jaw 强度调制放疗(F-IMRT)和切线部分容积调制弧形治疗(tP-VMAT)在同步双侧乳腺癌(SBBC)中的治疗计划。
对 12 例接受保乳手术后行全乳照射的 pTis-2N0M0 期 SBBC 患者,分别采用 F-IMRT 和 tP-VMAT 技术,将 42.56Gy(2.66Gy*16f)给予乳房。F-IMRT 采用 8-12 个 jaw-fixed 切线野,单(sF-IMRT)或双(F-IMRT)等中心位于胸骨下或左右计划靶区(PTV)中心,tP-VMAT 采用 4 个切线部分弧,两个等中心位于左右 PTV 中心。通过剂量体积直方图(DVH)分析评估计划。计算剂量学参数评估计划质量;总监测器单位(MU)和患者特异性质量保证(QA)的伽马分析也进行了评估。
对于 PTVs,三个计划的 D 和适形指数(CI)值相似。F-IMRT 根据 V 值显示出稍微更好的靶区覆盖率,并与 sF-IMRT 和 tP-VMAT 观察到的 V 和 D 值相比,显示出明显的降低。与 tP-VMAT 相比,sF-IMRT 在 V 、 V 和 D 方面略有优势。此外,F-IMRT 为 PTVs 实现了最佳的均匀性指数(HI)值。关于健康组织,tP-VMAT 具有最小化高剂量体积的优势。tP-VMAT 计划的 MU 分别比 sF-IMRT 和 F-IMRT 计划减少了约 1.45 倍和 1 倍,所有计划均通过 QA。对于肺部、心脏和肝脏,F-IMRT 在 D 值方面达到最小,与 tP-VMAT 相比有显著差异。同时,sF-IMRT 也优于 tP-VMAT。对于冠状动脉,tP-VMAT 达到最低的 D ,而 F-IMRT 比 sF-IMRT 低 2.24%。对于所有危险器官(OARs),tP-VMAT 在高剂量水平上具有优势。相比之下,sF-IMRT 和 F-IMRT 在低剂量水平上具有明显优势。sF-IMRT 和 F-IMRT 计划显示出一致的趋势。
所提供技术的所有治疗计划均质量较高,适用于 SBBC 患者。然而,我们建议优先选择单等中心 F-IMRT,因为它在 PTVs 中具有局部热点控制的巨大优势,并且在低剂量水平上降低了 OARs 的剂量。当肺部和心脏的照射剂量超过临床限制时,可以使用两个等中心 F-IMRT 来最大限度地减少 OAR 的保护。此外,当 PTVs 之间的间隔较窄时,可以采用 tP-VMAT 来改善 PTVs 的冷点或正常组织的高剂量暴露。