Bernasconi Paolo, Borsani Oscar
University of Pavia, Department of Molecular Medicine, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy.
J Oncol. 2019 Aug 7;2019:8323592. doi: 10.1155/2019/8323592. eCollection 2019.
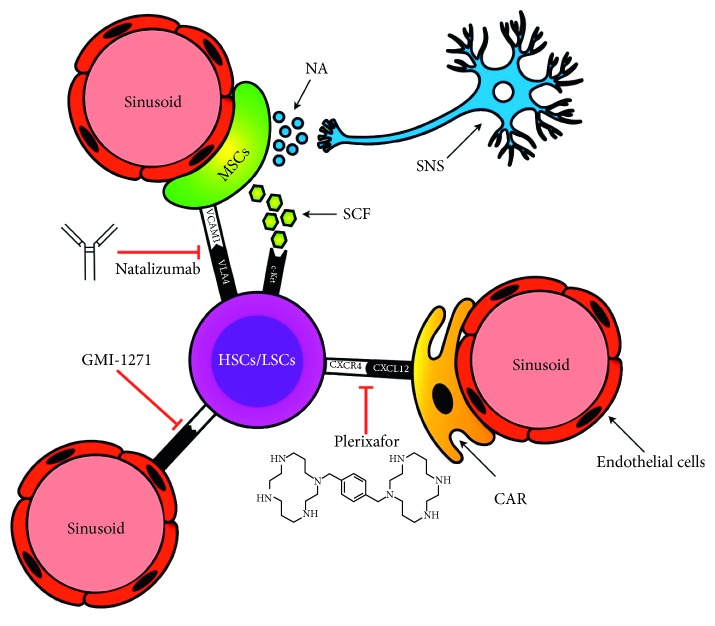
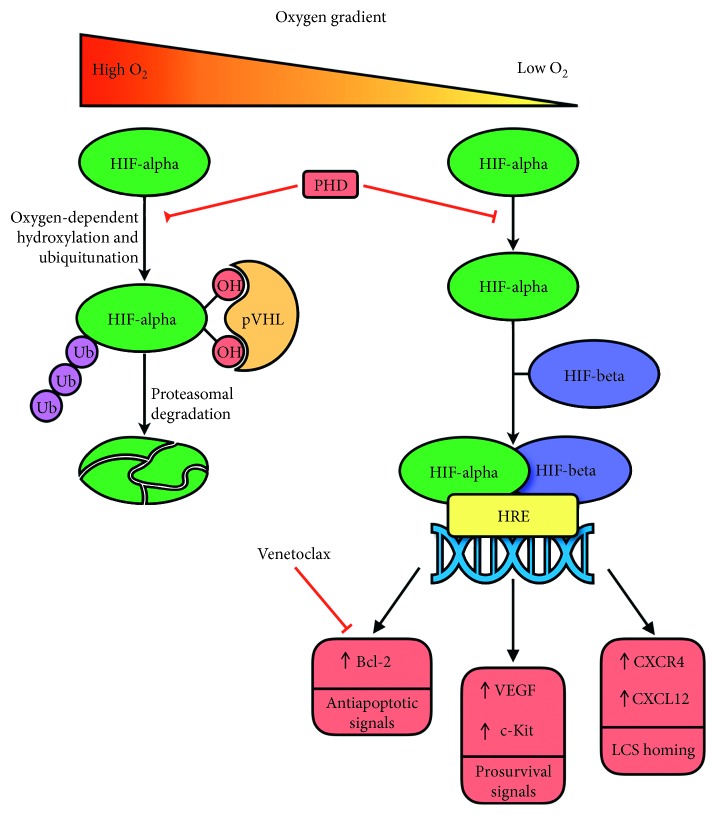
One of the most urgent needs in AML is to improve the disease cure rate as relapse still occurs in 60-80% of patients. Recent evidence suggests that dismal clinical outcomes may be improved by a better definition of the tight interaction between the AML cell population and the bone marrow (BM) microenvironment ("the niche"); the latter has been progressively highlighted to have an active role in the disease process. It has now been well established that the leukemic population may misinterpret niche-derived signals and remodel the niche, providing a shelter to AML cells and protecting them from the cytotoxic effects of chemoradiotherapy. Novel imaging technological advances and preclinical disease models have revealed that, due to the finite number of BM niches, leukemic stem cells (LSCs) and normal hematopoietic stem cells (HSCs) compete for the same functional areas. Thus, the removal of LSCs from the BM niche and the promotion of normal HSC engraftment should be the primary goals in antileukemic research. In addition, it is now becoming increasingly clear that AML-niche dynamics are disease stage specific. In AML, the niche has been linked to disease pathogenesis in the preleukemic stage, the niche becomes permissive once leukemic cells are established, and the niche is transformed into a self-reinforcing structure at a later disease stage. These concepts have been fostered by the demonstration that, in unrelated AML types, endosteal vessel loss occurs as a primary AML-induced niche alteration, and additional AML-induced alterations of the niche and normal hematopoiesis evolve focally and in parallel. Obviously, this endosteal vessel loss plays a fundamental role in AML pathogenesis by causing excessive vascular permeability, hypoxia, altered perfusion, and reduced drug delivery. Each of these alterations may be effectively targeted by various therapeutic procedures, but preservation of endosteal vessel integrity might be the best option for any future antileukemic treatment.
急性髓系白血病(AML)最迫切的需求之一是提高疾病治愈率,因为仍有60%-80%的患者会复发。最近的证据表明,通过更好地定义AML细胞群体与骨髓(BM)微环境(“生态位”)之间紧密的相互作用,可能会改善令人沮丧的临床结果;后者在疾病过程中的积极作用已逐渐得到重视。现已明确,白血病群体可能会误解来自生态位的信号并重塑生态位,为AML细胞提供庇护所,使其免受放化疗的细胞毒性作用。新的成像技术进展和临床前疾病模型表明,由于BM生态位数量有限,白血病干细胞(LSCs)和正常造血干细胞(HSCs)会竞争相同的功能区域。因此,从BM生态位中清除LSCs并促进正常HSC植入应是抗白血病研究的主要目标。此外,现在越来越清楚的是,AML-生态位动态具有疾病阶段特异性。在AML中,生态位在白血病前期与疾病发病机制相关,白血病细胞建立后生态位变得宽松,在疾病后期生态位转变为自我强化结构。这些概念得到了以下证据的支持:在不同类型的AML中,骨内膜血管丧失是AML诱导的主要生态位改变,AML诱导的生态位和正常造血的其他改变会局部且平行地演变。显然,这种骨内膜血管丧失通过导致血管通透性增加、缺氧、灌注改变和药物递送减少,在AML发病机制中起重要作用。这些改变中的每一种都可以通过各种治疗方法有效靶向,但保持骨内膜血管完整性可能是未来任何抗白血病治疗的最佳选择。