Roeleveld Peter Paul, Mendonca Malaika
Pediatric Intensive Care, Leiden University Medical Center, Leiden, Netherlands.
Pediatric Intensive Care Unit, Children's Hospital, Inselspital, Bern University Hospital, Bern, Switzerland.
Front Pediatr. 2019 Aug 21;7:327. doi: 10.3389/fped.2019.00327. eCollection 2019.
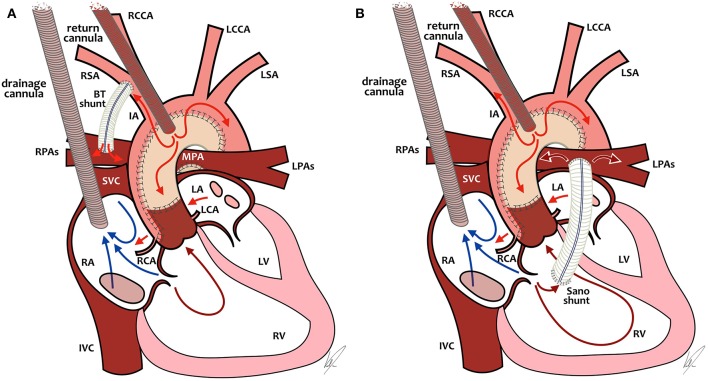
Worldwide, the use of Extracorporeal Membrane Oxygenation (ECMO) for cardiac failure has been steadily increasing in the neonatal population and has become a widely accepted modality. Especially in centers caring for children with (congenital) heart disease, ECMO is now an essential part of care available for those with severe heart failure as a bridge to recovery, long term mechanical support, or transplantation. Short-term outcomes depend very much on indication. Hospital survival is ~40% for all neonatal cardiac ECMO patients combined. ECMO is being used for pre- and/or post-operative stabilization in neonates with congenital heart disease and in neonates with medical heart disease such as myocarditis, cardiomyopathy or refractory arrhythmias. ECMO use during resuscitation (ECPR) or for sepsis is summarized elsewhere in this special edition of Frontiers in Pediatrics. In this review article, we will discuss the indications for neonatal cardiac ECMO, the difficult process of patients' selection and identifying the right timing to initiate ECMO, as well as outline pros and cons for peripheral vs. central cannulation. We will present predictors of mortality and, very importantly, predictors of survival: what can be done to improve the outcomes for your patients. Furthermore, an overview of current insights regarding supportive care in neonatal cardiac ECMO is given. Additionally, we will address issues specific to neonates with single ventricle physiology on ECMO, for example cannulation strategies and the influence of shunt type (Blalock-Taussig shunt vs. "right ventricle to pulmonary artery" shunt). We will not only focus on short term outcomes, such as hospital survival, but also on the importance of long-term neuro-developmental outcomes, and we will end this review with suggestions for future research.
在全球范围内,体外膜肺氧合(ECMO)在新生儿群体中用于治疗心力衰竭的应用一直在稳步增加,并已成为一种被广泛接受的治疗方式。特别是在照顾(先天性)心脏病患儿的中心,ECMO现在已成为治疗严重心力衰竭患儿的重要治疗手段,作为恢复、长期机械支持或移植的桥梁。短期预后很大程度上取决于适应症。所有接受新生儿心脏ECMO治疗的患者的医院生存率约为40%。ECMO被用于先天性心脏病新生儿以及患有心肌炎、心肌病或难治性心律失常等心脏疾病的新生儿术前和/或术后的稳定治疗。在复苏过程中使用ECMO(ECPR)或用于治疗脓毒症的情况在本期《儿科学前沿》的其他地方进行了总结。在这篇综述文章中,我们将讨论新生儿心脏ECMO的适应症、患者选择的困难过程以及确定启动ECMO的正确时机,同时概述外周插管与中心插管的优缺点。我们将介绍死亡率的预测因素,非常重要的是,还将介绍生存的预测因素:可以采取哪些措施来改善患者的预后。此外,还概述了目前关于新生儿心脏ECMO支持治疗的见解。此外,我们将讨论单心室生理的新生儿在接受ECMO治疗时的特殊问题,例如插管策略以及分流类型(Blalock-Taussig分流与“右心室至肺动脉”分流)的影响。我们不仅将关注短期预后,如医院生存率,还将关注长期神经发育预后的重要性,并且我们将在这篇综述的结尾提出未来研究的建议。