Poojary Shital, Miskeen Autar, Bagadia Jimish, Jaiswal Saurabh, Uppuluri Priya
Department of Dermatology and Venereology, K. J. Somaiya Hospital and Research Centre, Mumbai, Maharashtra, India.
DR Miskeen's Central Clinical Microbiology Laboratory, Thane, Maharashtra, India.
Indian J Dermatol. 2019 Jul-Aug;64(4):277-284. doi: 10.4103/ijd.IJD_456_18.
Recent years have seen an alarming rise in the prevalence of recalcitrant and relapsing dermatophyte infections in India associated with lack of clinical response to standard antifungal regimens.
A study was undertaken to identify the antifungal susceptibility patterns of dermatophyte species isolated from lesions of dermatophytoses in patients examined at our center.
A total of 85 patients with clinically diagnosed dermatophytoses were subjected to skin scrapings for potassium hydroxide mount (microscopic examination) and culture using Sabouraud's agar medium containing chloramphenicol and cycloheximide (incubated at 30°C). Antifungal susceptibilities [minimum inhibitory concentration-90 (MIC-90)] of the identified dermatophytes were tested for seven systemic and topical antifungal agents (terbinafine, griseofulvin, itraconazole, fluconazole, sertaconazole, ketoconazole, and clotrimazole) using Clinical and Laboratory Standards Institute broth microdilution method (M38-A).
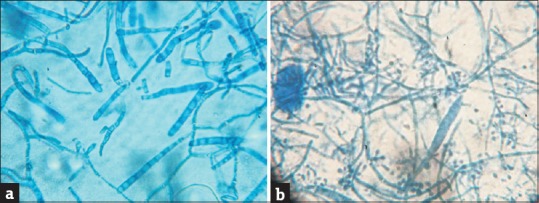
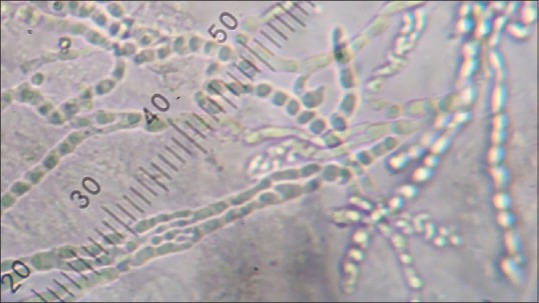
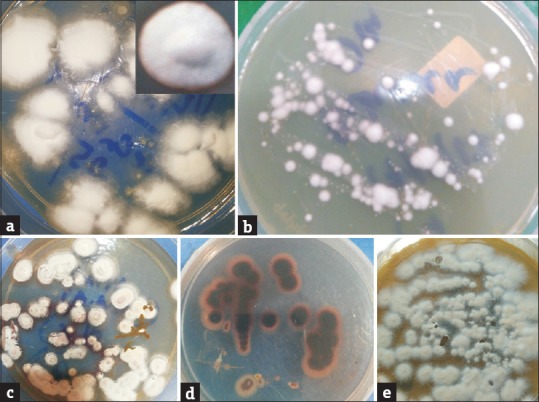
(50%) and (47.2%) were the two major species isolated. Isolates of both showed downy and granular forms (61.11%, 38.89% and 32.35%, 67.65%, respectively). The overall susceptibility profiles (MIC-90 ranges in μg/mL) of the seven drugs for and respectively were as follows: terbinafine (0.008-0256, 0.016-0.256), griseofulvin (0.03-1, 0.06-1), itraconazole (0.125-2, 0.25-2), fluconazole (0.125-1, 0.25-32), sertaconazole (0.03-1, 0.03-1), ketoconazole (0.06-1, 0.125-1), and clotrimazole (0.03-2, 0.06-1).
This study indicates a rising proportion of with increased proportion of granular form (). This study represents the current antifungal susceptibility profile of dermatophytic infections in a tertiary care medical center in western India with rising MICs to terbinafine and itraconazole.
近年来,印度顽固性和复发性皮肤癣菌感染的患病率惊人上升,这与对标准抗真菌治疗方案缺乏临床反应有关。
开展一项研究,以确定从我们中心接受检查的患者皮肤癣菌病皮损中分离出的皮肤癣菌种类的抗真菌药敏模式。
对85例临床诊断为皮肤癣菌病的患者进行皮肤刮屑,用于氢氧化钾涂片(显微镜检查),并使用含氯霉素和放线菌酮的沙氏琼脂培养基进行培养(在30°C孵育)。采用临床和实验室标准协会肉汤微量稀释法(M38 - A),对鉴定出的皮肤癣菌针对七种全身和局部抗真菌药物(特比萘芬、灰黄霉素、伊曲康唑、氟康唑、舍他康唑、酮康唑和克霉唑)进行抗真菌药敏试验[最低抑菌浓度-90(MIC-90)]。
分离出的两种主要菌种分别为(50%)和(47.2%)。两种菌种的分离株均显示出绒毛状和颗粒状形态(分别为61.11%,38.89%和32.35%,67.65%)。七种药物对和的总体药敏谱(MIC-90范围,μg/mL)如下:特比萘芬(0.008 - 0.256,0.016 - 0.256),灰黄霉素(0.03 - 1,0.06 - 1),伊曲康唑(0.125 - 2,0.25 - 2),氟康唑(0.125 - 1,0.25 - 32),舍他康唑(0.03 - 1,0.03 - 1),酮康唑(0.06 - 1,0.125 - 1),克霉唑(0.03 - 2,0.06 - 1)。
本研究表明菌种比例上升,颗粒状形态比例增加()。本研究代表了印度西部一家三级医疗中心皮肤癣菌感染的当前抗真菌药敏谱,对特比萘芬和伊曲康唑的MIC值不断上升。