Department of Neurology, Christian Doppler Medical Center, Paracelsus Medical University, Salzburg, Austria.
Research Institute for Neurointervention, Christian Doppler Medical Center, Paracelsus Medical University, Salzburg, Austria.
Sci Rep. 2019 Sep 13;9(1):13224. doi: 10.1038/s41598-019-49769-8.
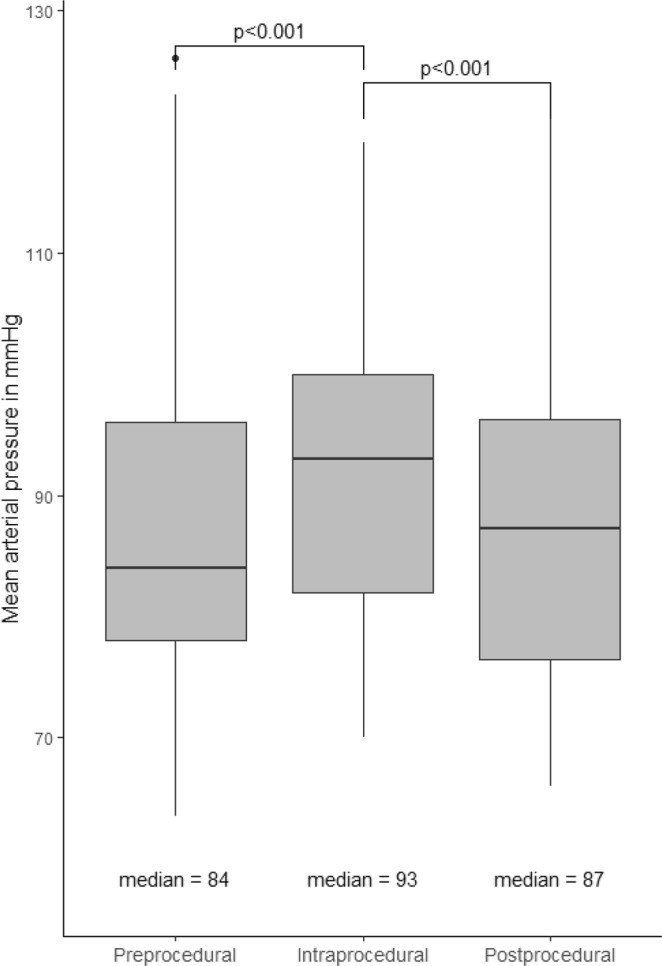
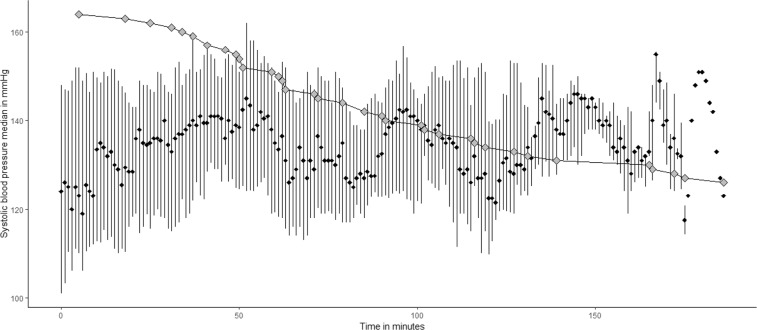
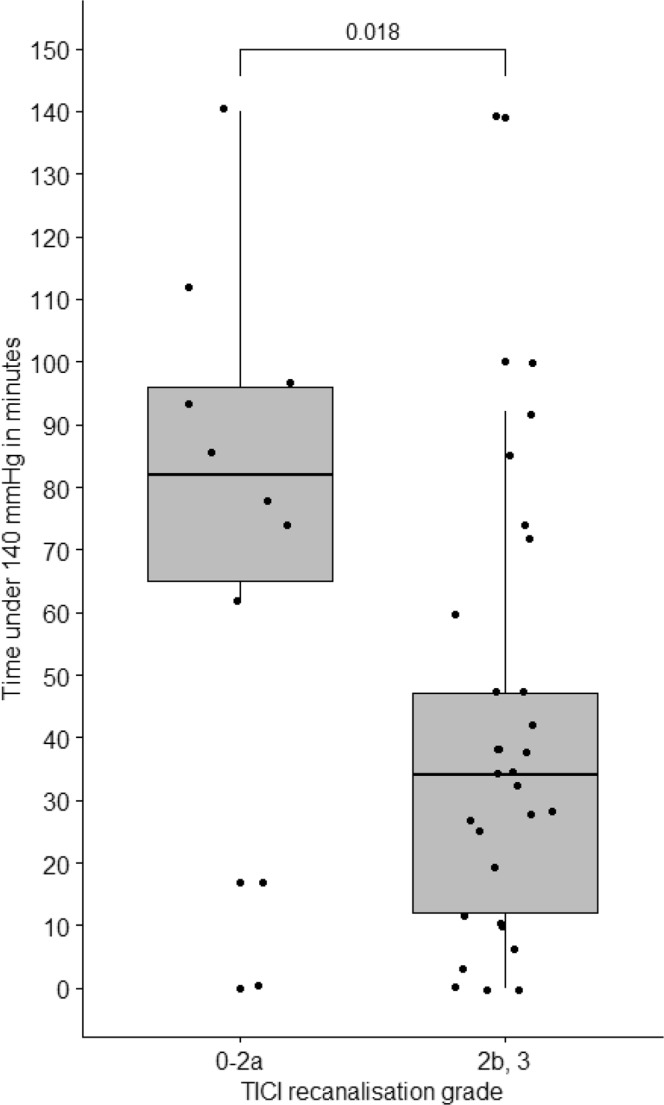
Acute basilar artery occlusion (BAO) is a rare but potentially life-threatening neurological condition. While endovascular therapy (EVT) has been shown to improve outcome, there is limited knowledge about prognostic factors beyond early recanalization. We studied whether blood pressure (BP) exceeds or falls below suggested thresholds during intervention and whether these changes are associated with complications and outcome. BP measurements mostly with one-minute intervals were available in 39 patients. An individual systolic blood pressure (SBP) reference value was defined as the median of the first five intra-procedural measurements. Half of the patients (51.3%) received drugs for BP augmentation and two a BP lowering drug (5.1%). Thrombolysis in cerebral infarction grade 2b and 3 (TICI) was achieved in 29 (74.4%) and 23 patients (58.9%) had good outcome at three months. We observed a continuous intra-procedural increase of median SBP (+11%) and mean arterial pressure (MAP, +10%, both p < 0.001), and a unique temporal pattern of intermittent peaks and troughs. Successful recanalization was more common in patients whose intra-procedural duration with SBP under 140 mmHg was shorter (p = 0.009). Patients with isolated tip of basilar artery (TBA) occlusion had significantly more BP excursion of 20% below the reference SBP and required more frequent use of sympathomimetic drugs compared to vertebrobasilar occlusion (p = 0.008 and p = 0.041, respectively). Brain hemorrhage was more prevalent in patients who experienced SBP excursions at least 20% above the individual reference value (p = 0.038) and a longer duration of time spent with SBP above 180 mmHg (p = 0.029). Patients with higher pre-procedural mean SBP had a greater chance of a good outcome (p = 0.03). This study using high resolution BP monitoring suggests a relationship between intra-procedural BP characteristics and recanalization, hemorrhagic complications and outcome in patients receiving EVT for acute posterior circulation cerebrovascular syndromes. Differences with regard to BP regulation during recanalization therapy for vertebrobasilar and TBA occlusion deserves further attention.
急性基底动脉闭塞(BAO)是一种罕见但潜在危及生命的神经系统疾病。虽然血管内治疗(EVT)已被证明可以改善预后,但对于早期再通以外的预后因素知之甚少。我们研究了介入治疗过程中血压(BP)是否超过或低于建议的阈值,以及这些变化是否与并发症和结果相关。39 例患者中有血压测量值,间隔大多为 1 分钟。个体收缩压(SBP)参考值定义为前五次术中测量的中位数。一半的患者(51.3%)接受了升压药物治疗,两名患者(5.1%)接受了降压药物治疗。29 例(74.4%)和 23 例(58.9%)患者达到了脑梗死溶栓 2b 级和 3 级(TICI),3 个月时预后良好。我们观察到术中 SBP (+11%)和平均动脉压(MAP,+10%)的中位数持续升高,且存在独特的间歇性波峰和波谷的时间模式。SBP 低于 140mmHg 的术中持续时间较短的患者,再通更常见(p<0.001)。单纯基底动脉尖端闭塞(TBA)患者的 SBP 参考值降低 20%的波动明显更多,且需要更频繁地使用拟交感神经药物,与椎基底动脉闭塞相比(p=0.008 和 p=0.041)。与 SBP 参考值至少升高 20%的患者相比,SBP 波动至少升高 20%的患者发生脑出血的可能性更大(p=0.038),且 SBP 高于 180mmHg 的时间更长(p=0.029)。术前平均 SBP 较高的患者有更好预后的机会(p=0.03)。本研究使用高分辨率 BP 监测,提示接受 EVT 治疗急性后循环脑血管综合征的患者,术中 BP 特征与再通、出血性并发症和结果之间存在关联。在椎基底动脉和 TBA 闭塞的再通治疗期间,BP 调节方面的差异值得进一步关注。