Department of Neurology, Christian Doppler Medical Center, Paracelsus Medical University, Ignaz-Harrer-Straße 79, 5020, Salzburg, Austria.
Department of Neurology, King's College Hospital, Denmark Hill, London, UK.
J Neuroinflammation. 2018 Nov 15;15(1):319. doi: 10.1186/s12974-018-1359-2.
The development of intracranial hemorrhage (ICH) in acute ischemic stroke is associated with a higher neutrophil to lymphocyte ratio (NLR) in peripheral blood. Here, we studied whether the predictive value of NLR at admission also translates into the occurrence of hemorrhagic complications and poor functional outcome after endovascular treatment (EVT).
We performed a retrospective analysis of consecutive patients with anterior circulation ischemic stroke who underwent EVT at a tertiary care center from 2012 to 2016. Follow-up scans were examined for non-procedural ICH and scored according to the Heidelberg Bleeding Classification. Demographic, clinical, and laboratory data were correlated with the occurrence of non-procedural ICH.
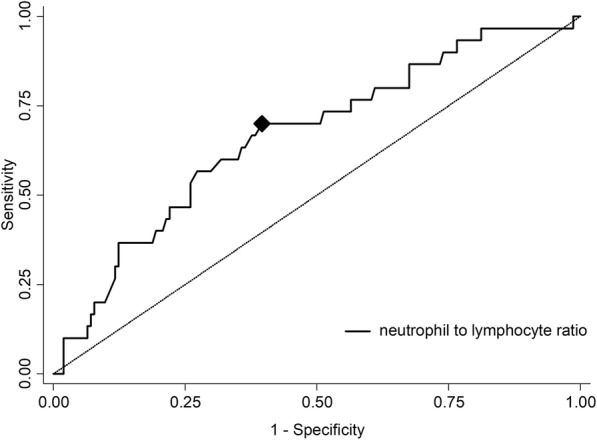
We identified 187 patients with a median age of 74 years (interquartile range [IQR] 60-81) and a median baseline National Institutes of Health Stroke scale (NIHSS) score of 18 (IQR 13-22). A bridging therapy with recombinant tissue-plasminogen activator (rt-PA) was performed in 133 (71%). Of the 31 patients with non-procedural ICH (16.6%), 13 (41.9%) were symptomatic. Patients with ICH more commonly had a worse outcome at 3 months (p = 0.049), and were characterized by a lower body mass index, more frequent presence of tandem occlusions, higher NLR, larger intracranial thrombus, and prolonged rt-PA and groin puncture times. In a multivariate analysis, higher admission NLR was independently associated with ICH (OR 1.09 per unit increase, 95% CI (1.00-1.20, p = 0.040). The optimal cutoff value of NLR that best distinguished the development of ICH was 3.89.
NLR is an independent predictor for the development of ICH after EVT. Further studies are needed to investigate the role of the immune system in hemorrhagic complications following EVT, and confirm the value of NLR as a potential biomarker.
急性缺血性脑卒中患者外周血中性粒细胞与淋巴细胞比值(NLR)升高与颅内出血(ICH)的发生有关。本研究旨在探讨入院时 NLR 的预测价值是否也能转化为血管内治疗(EVT)后出血并发症和不良功能结局的发生。
我们对 2012 年至 2016 年在一家三级护理中心接受 EVT 的前循环缺血性脑卒中连续患者进行了回顾性分析。通过随访扫描观察非程序 ICH 并根据海德堡出血分类进行评分。将人口统计学、临床和实验室数据与非程序 ICH 的发生相关联。
我们确定了 187 名年龄中位数为 74 岁(四分位距 [IQR] 60-81)且基线国立卫生研究院卒中量表(NIHSS)评分中位数为 18(IQR 13-22)的患者。133 名患者(71%)接受了重组组织型纤溶酶原激活剂(rt-PA)桥接治疗。在 31 名非程序 ICH 患者(16.6%)中,13 名(41.9%)为症状性 ICH。ICH 患者在 3 个月时更常见不良结局(p=0.049),其特征为 BMI 较低、更频繁出现串联闭塞、更高的 NLR、更大的颅内血栓形成以及 rt-PA 和腹股沟穿刺时间延长。多变量分析表明,入院时 NLR 升高与 ICH 独立相关(每单位增加 1.09,95%CI(1.00-1.20),p=0.040)。 NLR 最佳区分 ICH 发生的截断值为 3.89。
NLR 是 EVT 后 ICH 发生的独立预测因子。需要进一步研究以探讨免疫系统在 EVT 后出血并发症中的作用,并证实 NLR 作为潜在生物标志物的价值。