Departments of Cardiology and Cardiovascular Outcomes Research, Saint Luke's Mid America Heart Institute/University of Missouri-Kansas City, Kansas City, Missouri.
Department of Cardiology, Ahmanson-UCLA Cardiomyopathy Center, Ronald Reagan University of California Los Angeles Medical Center, Los Angeles, California.
JACC Heart Fail. 2019 Nov;7(11):933-941. doi: 10.1016/j.jchf.2019.05.016. Epub 2019 Sep 11.
This study sought to describe the short-term health status benefits of angiotensin-neprilysin inhibitor (ARNI) therapy in patients with heart failure and reduced ejection fraction (HFrEF).
Although therapy with sacubitril/valsartan, a neprilysin inhibitor, improved patients' health status (compared with enalapril) at 8 months in the PARADIGM-HF (Prospective Comparison of ARNI with ACE inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) study, the early impact of ARNI on patients' symptoms, functions, and quality of life is unknown.
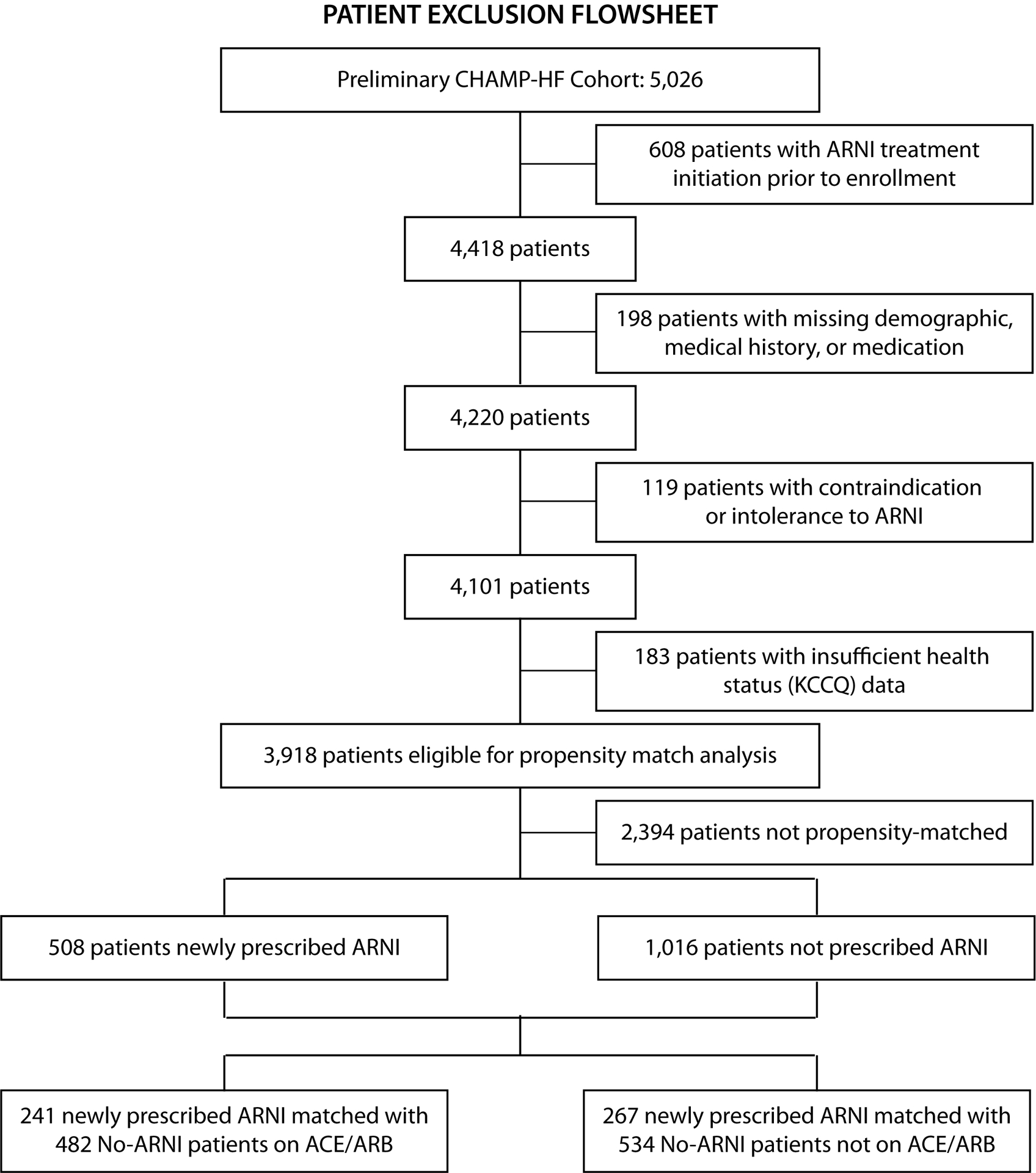
Health status was assessed by using the 12-item Kansas City Cardiomyopathy Questionnaire (KCCQ) in 3,918 outpatients with HFrEF and left ventricular ejection fraction ≤40% across 140 U.S. centers in the CHAMP-HF (Change the Management of Patients with Heart Failure) registry. ARNI therapy was initiated in 508 patients who were matched 1:2 to 1,016 patients who were not initiated on ARNI (no-ARNI), using a nonparsimonious time-dependent propensity score (6 sociodemographic factors, 23 clinical characteristics), prior KCCQ overall summary (KCCQ-OS) score, and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker status.
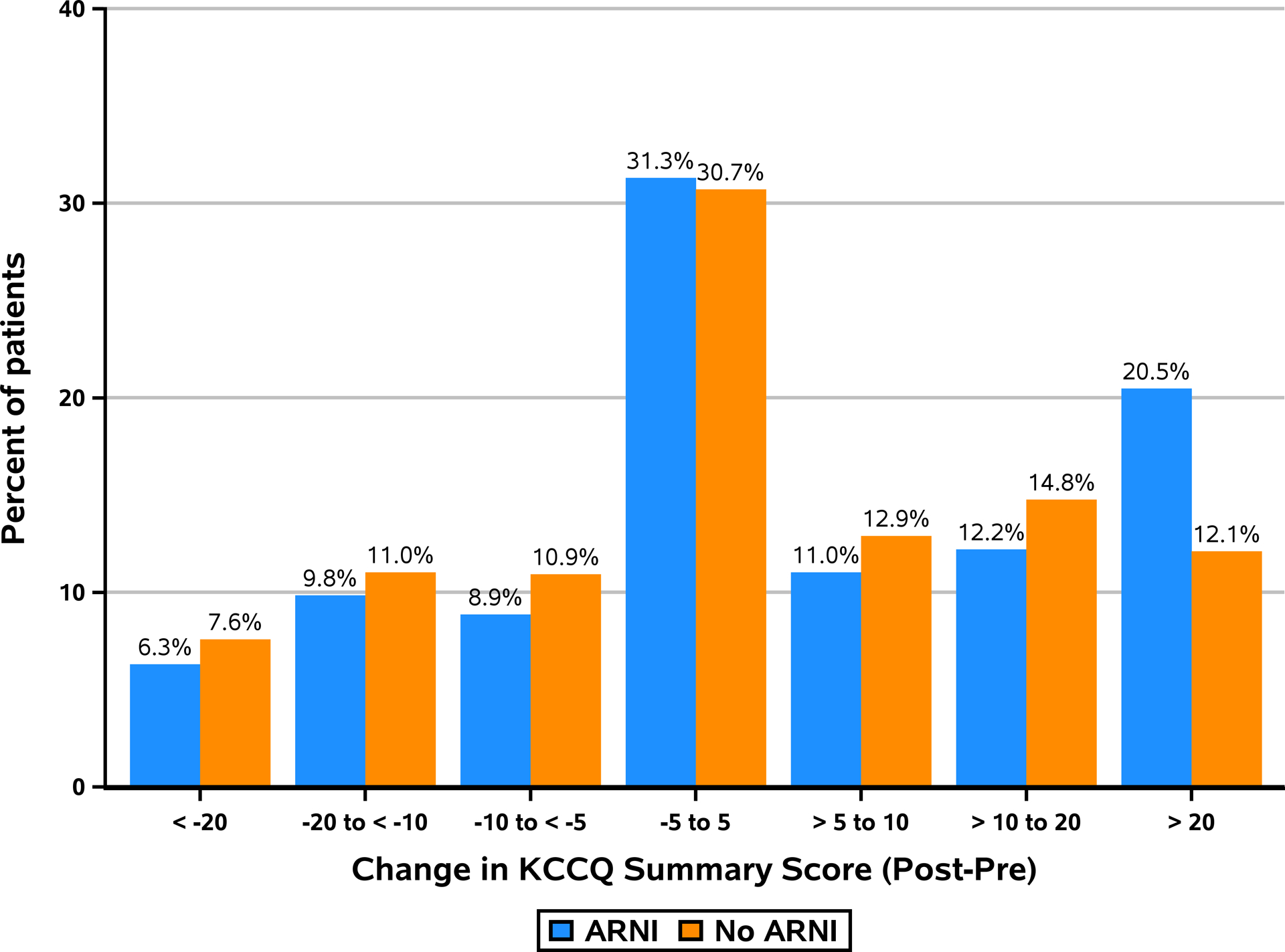
Multivariate linear regression demonstrated a greater mean improvement in KCCQ-OS in patients initiated on ARNI therapy (5.3 ± 19 vs. 2.5 ± 17.4, respectively; p < 0.001) over a median (interquartile range [IQR]) of 57 (32 to 104) days. The proportions of ARNI versus no-ARNI groups with ≥10-point (large) and ≥20-point (very large) improvements in KCCQ-OS were 32.7% versus 26.9%, respectively, and 20.5% versus 12.1%, respectively, consistent with numbers needed to treat of 18 and 12, respectively.
In routine clinical care, ARNI therapy was associated with early improvements in health status, with 20% experiencing a very large health status benefit compared with 12% who were not started on ARNI therapy. These findings support the use of ARNI to improve patients' symptoms, functions, and quality of life.
本研究旨在描述血管紧张素-脑啡肽酶抑制剂(ARNI)治疗射血分数降低的心力衰竭(HFrEF)患者的短期健康状况获益。
尽管在 PARADIGM-HF(血管紧张素受体脑啡肽酶抑制剂与血管紧张素转换酶抑制剂比较以确定对心力衰竭患者全球死亡率和发病率的影响)研究中,与依那普利相比,沙库巴曲缬沙坦(一种脑啡肽酶抑制剂)治疗 8 个月可改善患者的健康状况,但 ARNI 对患者症状、功能和生活质量的早期影响尚不清楚。
在 CHAMP-HF(改变心力衰竭患者管理)登记研究中,在美国 140 个中心的 3918 例 HFrEF 患者和左心室射血分数≤40%的患者中,使用 12 项堪萨斯城心肌病问卷(KCCQ)评估健康状况。在接受 ARNI 治疗的 508 例患者和未接受 ARNI 治疗的 1016 例患者(无 ARNI 组)中,采用非简约的时间依赖性倾向评分(6 个社会人口统计学因素,23 个临床特征)、之前的 KCCQ 综合评分(KCCQ-OS)和血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂的状态进行 1:2 匹配。
多变量线性回归显示,接受 ARNI 治疗的患者 KCCQ-OS 平均改善更大(分别为 5.3 ± 19 与 2.5 ± 17.4;p<0.001),中位(四分位距 [IQR])时间为 57(32 至 104)天。与无 ARNI 组相比,ARNI 组 KCCQ-OS 改善≥10 分(大)和≥20 分(非常大)的比例分别为 32.7%和 20.5%,分别为 26.9%和 12.1%,分别相当于需要治疗的人数为 18 和 12。
在常规临床护理中,ARNI 治疗与健康状况的早期改善相关,与未接受 ARNI 治疗的患者相比,20%的患者健康状况得到了非常大的改善,而 12%的患者健康状况得到了改善。这些发现支持使用 ARNI 改善患者的症状、功能和生活质量。