Greenberg Barry
Sulpizio Family Cardiovascular Center and University of California, San Diego Medical Center, La Jolla, CA, USA.
Int J Heart Fail. 2020 Mar 24;2(2):73-90. doi: 10.36628/ijhf.2020.0002. eCollection 2020 Apr.
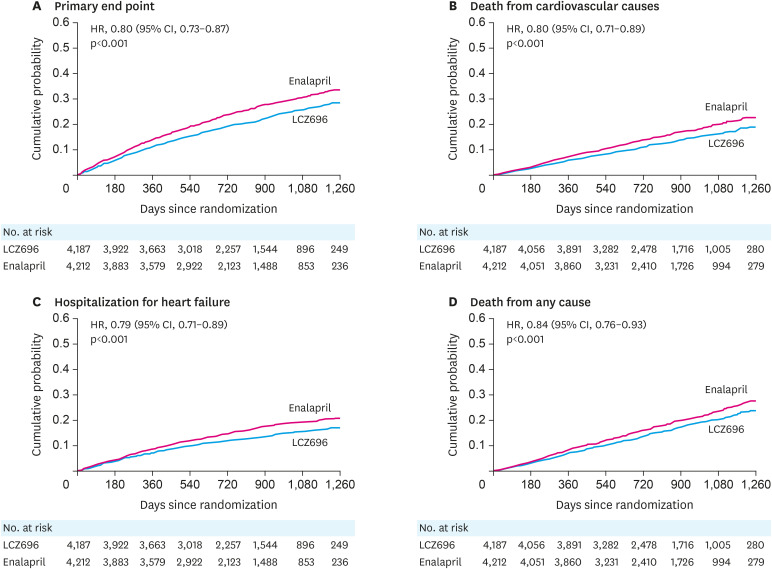
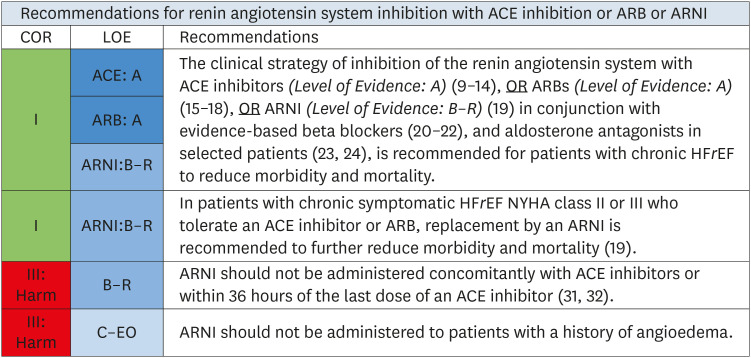
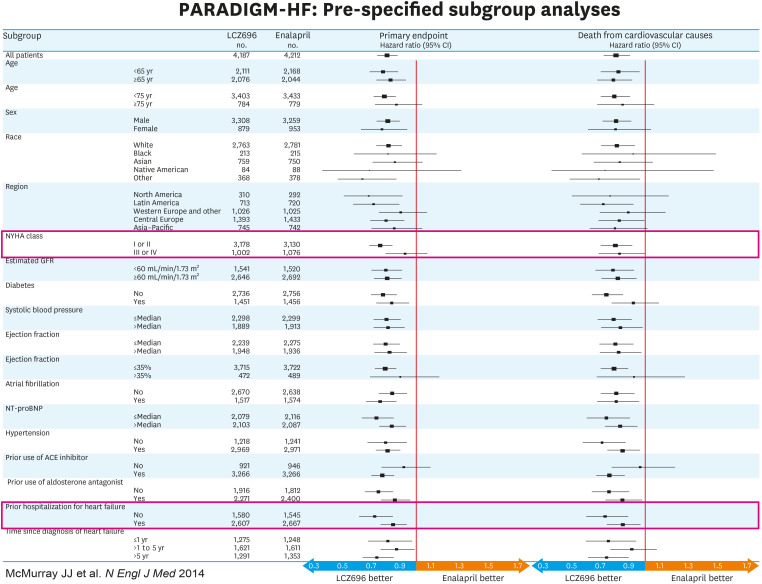
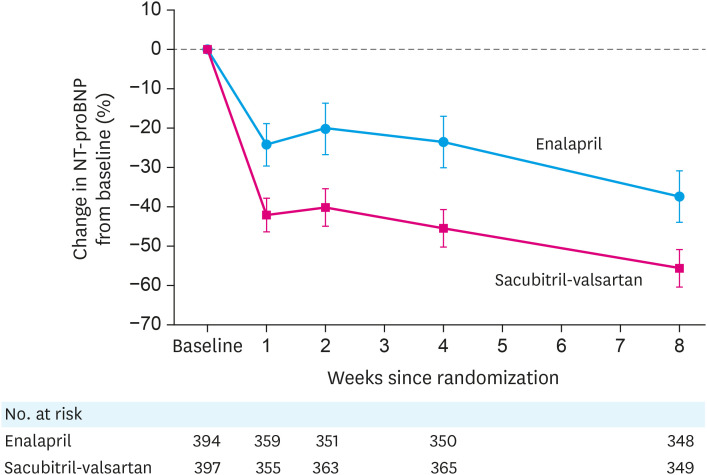
Recognition that neurohormonal activation plays a central role in the pathogenesis of heart failure (HF) led to the development of angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers, mineralocorticoid receptor antagonists and beta blockers. While there has been substantial success with these neurohormonal blocking drugs in patients with HF with reduced ejection fraction (HFrEF), persistently high rates of morbidity and mortality in this population underscore the need for more effective therapies. As part of the systemic neurohormonal activation that takes place in patients with HF, systems that counteract the adverse effect of the renin angiotensin aldosterone system (RAAS) and sympathetic nervous system (SNS) are also activated. Evidence that neprilysin metabolizes many of the effector molecules produced by these counter-regulatory systems raised the possibility that inhibition of this enzyme might be beneficial. However, since angiotensin II is a substrate of neprilysin, inhibition of the enzyme alone would increase levels of this peptide. Thus, treatment strategies that combine RAAS blockade with neprilysin inhibition were sought. Recent large scale randomized clinical trials (RCTs) have provided compelling evidence that sacubitril-valsartan, an angiotensin receptor-neprilysin inhibitor (ARNI), is superior to an ACEI in reducing mortality and HF hospitalization and in improving quality of life in patients with stage C HFrEF. In these trials, sacubitril-valsartan was found to be safe and well tolerated. This review presents the rationale for using ARNIs, describes the RCTs showing their efficacy, summarizes updated recommendations from recent guidelines, and provides practical points about ARNI initiation and up-titration.
认识到神经激素激活在心力衰竭(HF)发病机制中起核心作用,促使了血管紧张素转换酶抑制剂(ACEIs)、血管紧张素受体阻滞剂、盐皮质激素受体拮抗剂和β受体阻滞剂的研发。虽然这些神经激素阻断药物在射血分数降低的心力衰竭(HFrEF)患者中取得了显著成功,但该人群中持续居高不下的发病率和死亡率凸显了对更有效治疗方法的需求。作为HF患者全身神经激素激活的一部分,抵消肾素血管紧张素醛固酮系统(RAAS)和交感神经系统(SNS)不良反应的系统也被激活。有证据表明,中性肽链内切酶可代谢这些反调节系统产生的许多效应分子,这增加了抑制该酶可能有益的可能性。然而,由于血管紧张素II是中性肽链内切酶的一种底物,单独抑制该酶会增加这种肽的水平。因此,人们寻求将RAAS阻断与中性肽链内切酶抑制相结合的治疗策略。最近的大规模随机临床试验(RCTs)提供了令人信服的证据,表明血管紧张素受体 - 中性肽链内切酶抑制剂(ARNI)沙库巴曲缬沙坦在降低C期HFrEF患者的死亡率和HF住院率以及改善生活质量方面优于ACEI。在这些试验中,发现沙库巴曲缬沙坦安全且耐受性良好。本综述阐述了使用ARNI的基本原理,描述了显示其疗效的RCTs,总结了近期指南的更新建议,并提供了关于ARNI起始和滴定的实用要点。