Ridgely M Susan, Duffy Erin, Wolf Laura, Vaiana Mary, Scanlon Dennis, Buttorff Christine, Leitzell Brigitt, Ahluwalia Sangeeta, Hilton Lara, Agniel Denis, Haviland Amelia, Damberg Cheryl L
RAND Corporation, US.
Pennsylvania State University, US.
EGEMS (Wash DC). 2019 Aug 2;7(1):39. doi: 10.5334/egems.302.
As hospitals and physician organizations increasingly vertically integrate, there is an important opportunity to use health systems to improve performance. Prior research has largely relied on secondary data sources, but little is known about how health systems are organized "on the ground" and what mechanisms are available to influence physician practice at the front line of care.
We collected in-depth information on eight health systems through key informant interviews, descriptive surveys, and document review. Qualitative data were systematically coded. We conducted analyses to identify organizational structures and mechanisms through which health systems influence practice.
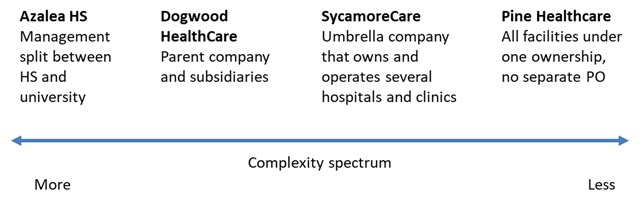
As expected, we found that health systems vary on multiple dimensions related to organizational structure (e.g., size, complexity) which reflects history, market and mission. With regard to levers of influence, we observed within-system variation both in mechanisms (e.g., employment of physicians, system-wide EHR, standardization of service lines) and level of influence. Concepts such as "core" versus "peripheral" were more salient than "ownership" versus "contract."
Data from secondary sources can help identify and map health systems, but they do not adequately describe them or the variation that exists within and across systems. To examine the degree to which health systems can influence performance, more detailed and nuanced information on health system characteristics is necessary.
The mixed-methods data accrual approach used in this study provides granular qualitative data that enables researchers to describe multi-layered health systems, grasp the context in which they operate, and identify the key drivers of performance.
随着医院和医师组织日益纵向整合,利用卫生系统来提高绩效存在重要机遇。先前的研究很大程度上依赖二手数据源,但对于卫生系统在实际中是如何组织的,以及在一线医疗中影响医师实践的机制却知之甚少。
我们通过关键信息人访谈、描述性调查和文件审查收集了八个卫生系统的深入信息。对定性数据进行了系统编码。我们进行分析以确定卫生系统影响实践的组织结构和机制。
正如预期的那样,我们发现卫生系统在与组织结构相关的多个维度上存在差异(例如规模、复杂性),这反映了历史、市场和使命。关于影响杠杆,我们观察到系统内部在机制(例如医师雇佣、全系统电子健康记录、服务线标准化)和影响程度方面都存在差异。“核心”与“外围”等概念比“所有权”与“合同”更为突出。
来自二手数据源的数据有助于识别和描绘卫生系统,但它们无法充分描述这些系统或系统内部及之间存在的差异。为了研究卫生系统能够影响绩效的程度,需要关于卫生系统特征的更详细和细致入微的信息。
本研究中使用的混合方法数据收集方法提供了详细的定性数据,使研究人员能够描述多层次的卫生系统,把握其运作背景,并确定绩效的关键驱动因素。