RAND Corporation, Santa Monica, California and Boston, Massachusetts.
Division of General Internal Medicine and Primary Care, Brigham and Women's Hospital, Boston, Massachusetts.
JAMA Health Forum. 2022 Jan 28;3(1):e214634. doi: 10.1001/jamahealthforum.2021.4634. eCollection 2022 Jan.
Public and private payers continue to expand use of alternative payment models, aiming to use value-based payment to affect the care delivery of their contracted health system partners. In parallel, health systems and their employment of physicians continue to grow. However, the degree to which health system physician compensation reflects an orientation toward value, rather than volume, is unknown.
To characterize primary care physician (PCP) and specialist compensation arrangements among US health system-affiliated physician organizations (POs) and measure the portion of total physician compensation based on quality and cost performance.
This study was a cross-sectional mixed-methods analysis of in-depth multimodal data (compensation document review, interviews with 40 PO leaders, and surveys conducted between November 2017 and July 2019) from 31 POs affiliated with 22 purposefully selected health systems in 4 states. Data were analyzed from June 2019 to September 2020.
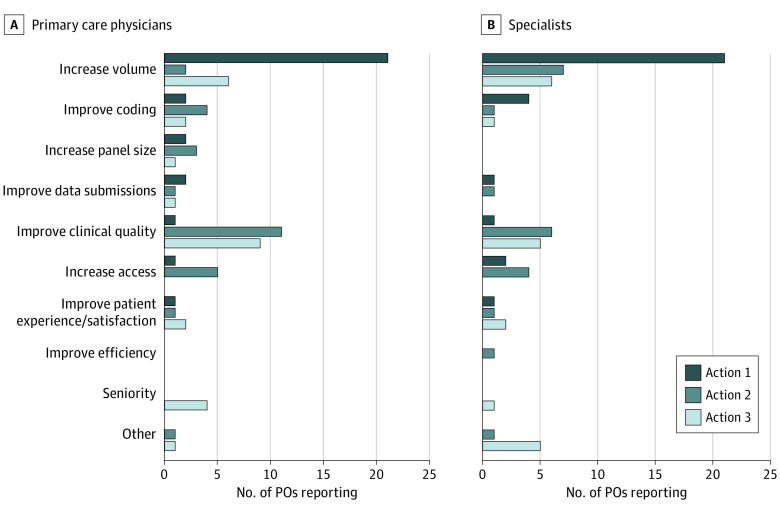
The frequency of PCP and specialist compensation types and the percentage of compensation when included, including base compensation incentives, quality and cost performance incentives, and other financial incentives. The top 3 actions physicians could take to increase their compensation. The association between POs' percentage of revenue from fee-for-service and their physicians' volume-based compensation percentage.
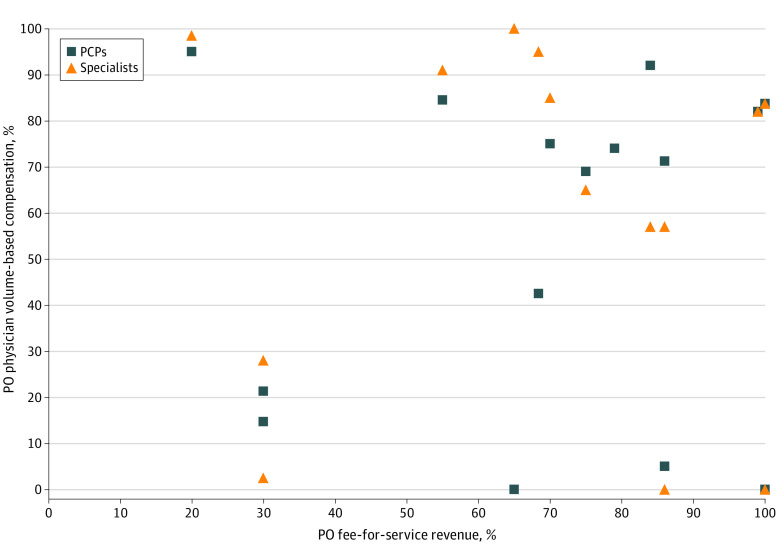
Volume-based compensation was the most common base compensation incentive component for PCPs (26 POs [83.9%]; mean, 68.2% of compensation; median, 81.4%; range, 5.0%-100.0% when included) and specialists (29 POs [93.3%]; mean, 73.7% of compensation; median, 90.5%; range, 2.5%-100.0% when included). While quality and cost performance incentives were common (included by 83.9%-56.7% of POs for PCPs and specialists, respectively), the percentage of compensation based on quality and cost performance was modest (mean, 9.0% [median, 8.3%; range, 1.0%-25.0%] for PCPs and 5.3% [median, 4.5%; range, 0.5%-16.0%] for specialists when included). Increasing the volume of services was the most commonly cited action for physicians to increase compensation, reported as the top action by 22 POs (70.0%) for PCPs and specialists. We observed a very weak, nonsignificant association between the percentage of revenue of POs from fee for service and the PCP and specialist volume-based compensation percentage ( = 0.08; = .78 and = -0.04; = .89, respectively).
The results of this cross-sectional study suggest that PCPs and specialists despite receiving value-based reimbursement incentives from payers, the compensation of health system PCPs and specialists was dominated by volume-based incentives designed to maximize health systems revenue.
公共和私人支付者继续扩大使用替代支付模式,旨在利用基于价值的支付来影响其签约医疗系统合作伙伴的医疗服务提供。与此同时,医疗系统及其对医生的雇佣规模继续扩大。然而,医疗系统医生薪酬反映出对价值(而非数量)的重视程度尚不清楚。
描述美国医疗系统附属医师组织(PO)中初级保健医生(PCP)和专家的薪酬安排,并衡量基于质量和成本绩效的医生总薪酬部分。
设计、设置和参与者:这是一项横断面混合方法分析,使用了来自 4 个州的 22 个有目的选择的医疗系统中 31 个 PO 的深入多模态数据(薪酬文件审查、对 40 个 PO 领导者的访谈以及 2017 年 11 月至 2019 年 7 月之间进行的调查)。数据于 2019 年 6 月至 2020 年 9 月进行分析。
PCP 和专家薪酬类型的频率,以及包含的薪酬百分比,包括基本工资激励、质量和成本绩效激励以及其他财务激励。医生可以采取的增加薪酬的前 3 项行动。PO 从按服务收费获得的收入百分比与其医生基于数量的薪酬百分比之间的关联。
基于数量的薪酬是 PCP(26 个 PO [83.9%];平均占薪酬的 68.2%;中位数为 81.4%;范围为 5.0%-100.0%,包含在内)和专家(29 个 PO [93.3%];平均占薪酬的 73.7%;中位数为 90.5%;范围为 2.5%-100.0%,包含在内)的最常见基本工资激励组成部分。虽然质量和成本绩效激励很常见(分别有 83.9%-56.7%的 PO 为 PCP 和专家提供),但基于质量和成本绩效的薪酬百分比适中(平均占 PCP 的 9.0%[中位数为 8.3%;范围为 1.0%-25.0%]和专家的 5.3%[中位数为 4.5%;范围为 0.5%-16.0%],包含在内)。增加服务量是医生增加薪酬的最常被提及的行动,有 22 个 PO(70.0%)报告了这是 PCP 和专家的首要行动。我们观察到 PO 从按服务收费获得的收入百分比与 PCP 和专家基于数量的薪酬百分比之间存在非常弱的、无统计学意义的关联( = 0.08; = .78 和 = -0.04; = .89,分别)。
这项横断面研究的结果表明,尽管 PCP 和专家从支付者那里获得了基于价值的报销激励,但医疗系统的 PCP 和专家薪酬主要由旨在最大化医疗系统收入的基于数量的激励措施主导。