Department of General Surgery (Emergency Surgery), Fujian Medical University Union Hospital, Fuzhou 350001, Fujian Province, China.
Immunotherapy Institute, Fujian Medical University, Fuzhou 350122, Fujian Province, China.
World J Gastroenterol. 2019 Sep 7;25(33):4970-4984. doi: 10.3748/wjg.v25.i33.4970.
Obstructive colorectal cancer (OCC) is always accompanied by severe complications, and the optimal strategy for patients with OCC remains undetermined. Different from emergency surgery (ES), self-expandable metal stents (SEMS) as a bridge to surgery (BTS), could increase the likelihood of primary anastomosis. However, the stent failure and related complications might give rise to a high recurrence rate. Few studies have focused on the indications for either method, and the relationship between preoperative inflammation indexes and the prognosis of OCC is still underestimated.
To explore the indications for ES and BTS in OCCs based on preoperative inflammation indexes.
One hundred and twenty-eight patients who underwent ES or BTS from 2008 to 2015 were enrolled. Receiver operating characteristic (ROC) curve analysis was used to define the optimal preoperative inflammation index and its cutoff point. Kaplan-Meier analyses and Cox proportional hazards models were applied to assess the association between the preoperative inflammation indexes and the survival outcomes [overall survival (OS) and disease-free survival (DFS)]. Stratification analysis was performed to identify the subgroups that would benefit from ES or BTS.
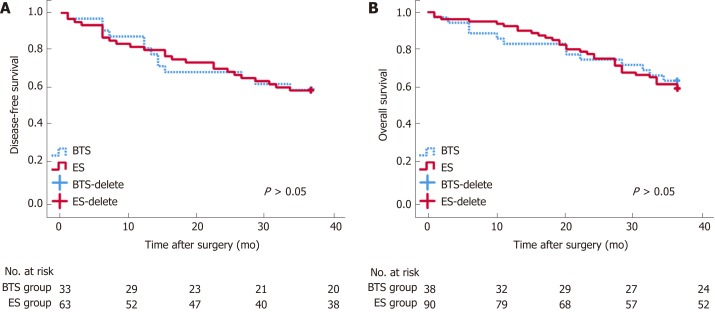
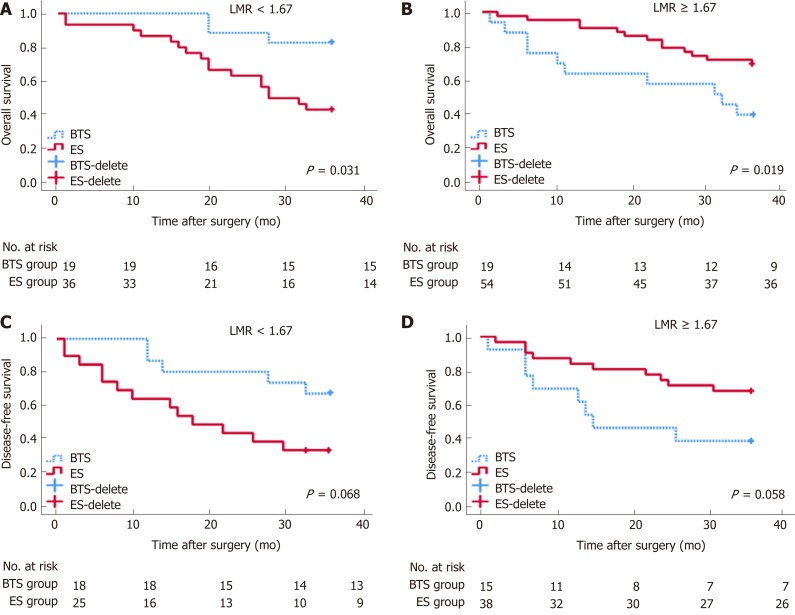
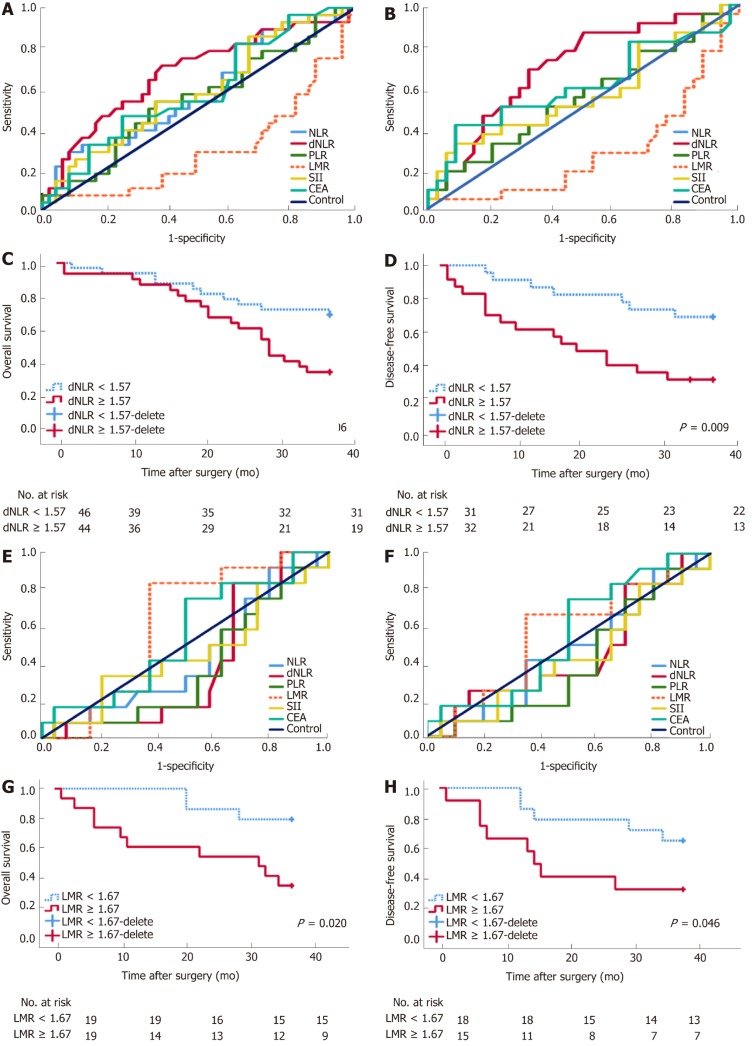
OS and DFS were comparable between the ES and BTS groups ( > 0.05). ROC curve analysis showed derived neutrophil-to-lymphocyte ratio (dNLR) as the optimal biomarker for the prediction of DFS in ES ( < 0.05). Lymphocyte-to-monocyte ratio (LMR) was recommended for BTS with regard to OS and DFS ( < 0.05). dNLR was related to stoma construction ( = 0.001), pneumonia ( = 0.054), and DFS ( = 0.009) in ES. LMR was closely related to lymph node invasion (LVI) ( = 0.009), OS ( = 0.020), and DFS ( = 0.046) in the BTS group. dNLR was an independent risk factor for ES in both OS ( = 0.032) and DFS ( = 0.016). LMR affected OS ( = 0.053) and DFS ( = 0.052) in the BTS group. LMR could differentiate the OS between the ES and BTS groups ( < 0.05).
Preoperative dNLR and LMR could predict OS and DFS in patients undergoing ES and BTS, respectively. For OCC, as the potential benefit group, patients with a low LMR might be preferred for BTS SEMS insertion.
阻塞性结直肠癌(OCC)常伴有严重并发症,OCC 患者的最佳治疗策略仍未确定。与急诊手术(ES)不同,自膨式金属支架(SEMS)作为桥接手术(BTS)可以增加一期吻合的可能性。然而,支架失败和相关并发症可能导致高复发率。很少有研究关注这两种方法的适应证,术前炎症指标与 OCC 预后的关系仍被低估。
基于术前炎症指标探讨 ES 和 BTS 在 OCC 中的适应证。
纳入 2008 年至 2015 年接受 ES 或 BTS 的 128 例患者。采用受试者工作特征(ROC)曲线分析确定最佳术前炎症指标及其截断值。Kaplan-Meier 分析和 Cox 比例风险模型用于评估术前炎症指标与生存结局(总生存(OS)和无病生存(DFS))之间的关系。进行分层分析以确定从 ES 或 BTS 中获益的亚组。
ES 和 BTS 组之间的 OS 和 DFS 无显著差异(>0.05)。ROC 曲线分析显示,中性粒细胞与淋巴细胞比值(dNLR)是 ES 预测 DFS 的最佳生物标志物(<0.05)。淋巴细胞与单核细胞比值(LMR)推荐用于 BTS 的 OS 和 DFS(<0.05)。dNLR 与造口术(=0.001)、肺炎(=0.054)和 DFS(=0.009)有关在 ES 中。LMR 与淋巴结侵犯(LVI)(=0.009)、OS(=0.020)和 DFS(=0.046)密切相关在 BTS 组中。dNLR 是 OS(=0.032)和 DFS(=0.016)中 ES 的独立危险因素。LMR 影响 BTS 组的 OS(=0.053)和 DFS(=0.052)。LMR 可以区分 ES 和 BTS 组之间的 OS(<0.05)。
术前 dNLR 和 LMR 可分别预测 ES 和 BTS 患者的 OS 和 DFS。对于 OCC,作为潜在受益组,低 LMR 患者可能更适合 BTS 放置 SEMS。