Department of Cardiology, Medical Clinic I, University Hospital of the RWTH Aachen, Pauwelsstr. 30, 52074, Aachen, Germany.
Zoological Institute, Department of Cell- and Neurobiology, Karlsruhe Institute of Technology (KIT), Karlsruhe, Germany.
Cardiovasc Diabetol. 2019 Sep 24;18(1):122. doi: 10.1186/s12933-019-0926-x.
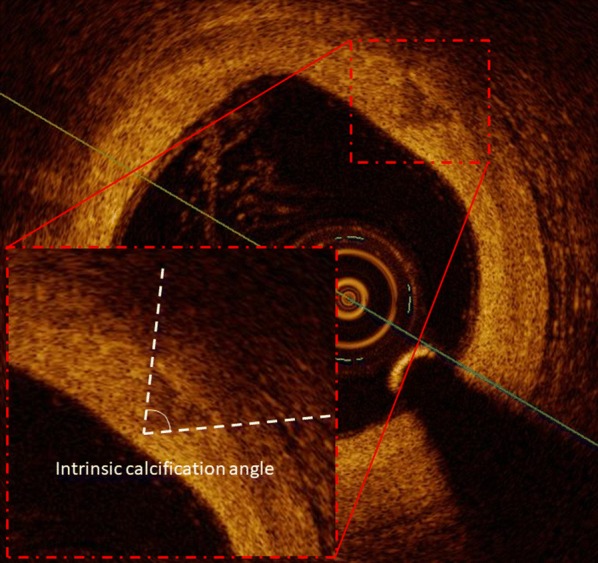
Coronary calcification is associated with high risk for cardiovascular events. However, its impact on plaque vulnerability is incompletely understood. In the present study we defined the intrinsic calcification angle (ICA) as the angle externally projected by a vascular calcification and analyzed its role as novel feature of coronary plaque vulnerability in patients with type 2 diabetes.
Optical coherence tomography was used to determine ICA in 219 calcifications from 56 patients with stable coronary artery disease (CAD) and 143 calcifications from 36 patients with acute coronary syndrome (ACS). We then used finite elements analysis to gain mechanistic insight into the effects of ICA.
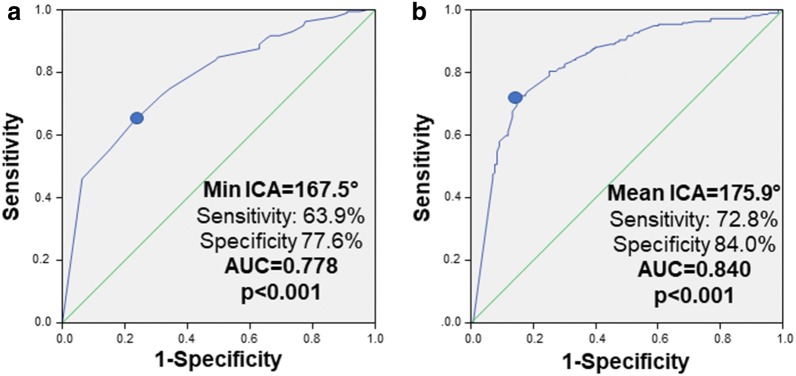
Minimal (139.8 ± 32.8° vs. 165.6 ± 21.6°, p < 0.001) and mean ICA (164.1 ± 14.3° vs. 176.0 ± 8.4°, p < 0.001) were lower in ACS vs. stable CAD patients. Mean ICA predicted ACS with very good diagnostic efficiency (AUC = 0.840, 95% CI 0.797-0.882, p < 0.001, optimal cut-off 175.9°); younger age (OR 0.95 per year, 95% CI 0.92-0.98, p = 0.002), male sex (OR 2.18, 95% CI 1.41-3.38, p < 0.001), lower HDL-cholesterol (OR 0.82 per 10 mg/dl, 95% CI 0.68-0.98, p = 0.029) and ACS (OR 14.71, 95% CI 8.47-25.64, p < 0.001) were determinants of ICA < 175.9°. A lower ICA predicted ACS (OR for 10°-variation 0.25, 95% CI 0.13-0.52, p < 0.001) independently from fibrous cap thickness, presence of macrophages or extension of lipid core. In finite elements analysis we confirmed that lower ICA causes increased stress on a lesion's fibrous cap; this effect was potentiated in more superficial calcifications and adds to the destabilizing role of smaller calcifications.
Our clinical and mechanistic data for the first time identify ICA as a novel feature of coronary plaque vulnerability.
冠状动脉钙化与心血管事件的高风险相关。然而,其对斑块易损性的影响尚不完全清楚。在本研究中,我们将血管钙化的外部投影角度定义为固有钙化角(ICA),并分析了其在 2 型糖尿病患者中作为冠状动脉斑块易损性新特征的作用。
使用光学相干断层扫描(OCT)确定 56 例稳定型冠状动脉疾病(CAD)患者的 219 个钙化灶和 36 例急性冠状动脉综合征(ACS)患者的 143 个钙化灶的 ICA。然后,我们使用有限元分析来深入了解 ICA 的影响。
ACS 患者的最小 ICA(139.8±32.8° vs. 165.6±21.6°,p<0.001)和平均 ICA(164.1±14.3° vs. 176.0±8.4°,p<0.001)均低于稳定 CAD 患者。平均 ICA 对 ACS 具有非常好的诊断效率(AUC=0.840,95%CI 0.797-0.882,p<0.001,最佳截断值 175.9°);年龄较小(每年 0.95,95%CI 0.92-0.98,p=0.002)、男性(OR 2.18,95%CI 1.41-3.38,p<0.001)、较低的高密度脂蛋白胆固醇(每 10mg/dl 0.82,95%CI 0.68-0.98,p=0.029)和 ACS(OR 14.71,95%CI 8.47-25.64,p<0.001)是 ICA<175.9°的决定因素。较低的 ICA 预测 ACS(每 10°变化的 OR 0.25,95%CI 0.13-0.52,p<0.001)独立于纤维帽厚度、巨噬细胞存在或脂质核心延伸。在有限元分析中,我们证实较低的 ICA 会导致病变纤维帽上的应力增加;这种效应在更浅层的钙化中更为明显,并增加了较小钙化的不稳定性作用。
我们的临床和机制数据首次将 ICA 确定为冠状动脉斑块易损性的一个新特征。