Hospital Espírito Santo de Évora, Évora - Portugal.
Centro Nacional Coleção de Dados em Cardiologia, Coimbra - Portugal.
Arq Bras Cardiol. 2019 Nov;113(5):948-957. doi: 10.5935/abc.20190190.
New-onset atrial fibrillation complicating acute myocardial infarction represents an important challenge, with prognostic significance.
To study the incidence, impact on therapy and mortality, and to identify predictors of development of new-onset atrial fibrillation during hospital stay for ST-segment elevation myocardial infarction.
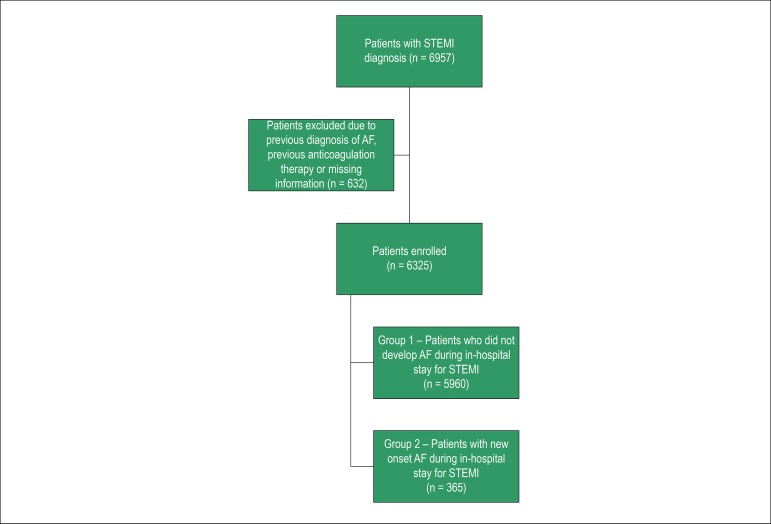
We studied all patients with ST-elevation myocardial infarction included consecutively, between 2010 and 2017, in a Portuguese national registry and compared two groups: 1 - no atrial fibrillation and 2 - new-onset atrial fibrillation. We adjusted a logistic regression model data analysis to assess the impact of new-onset atrial fibrillation on in-hospital mortality and to identify independent predictors of its development. A p value < 0.05 was considered significant.
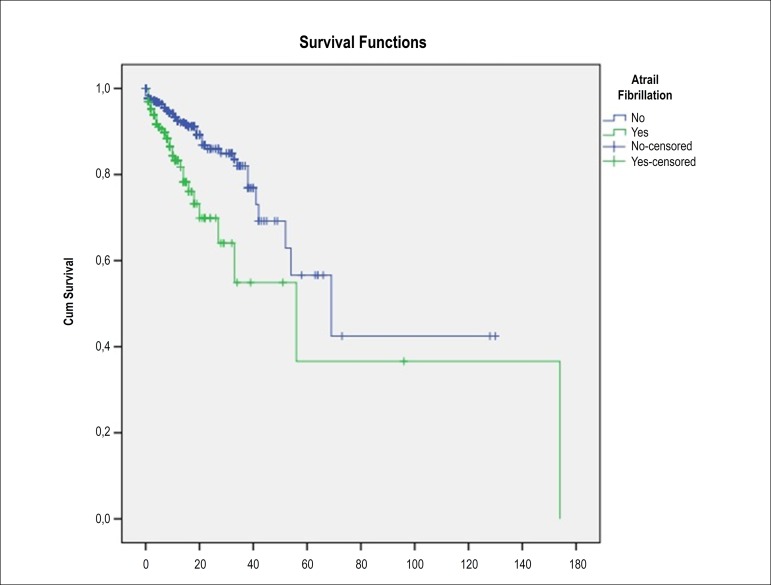
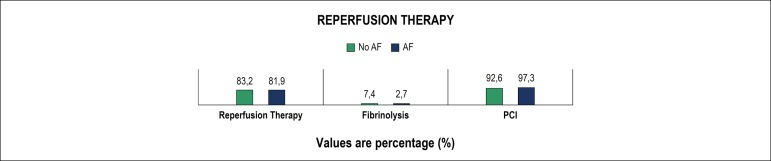
We studied 6325 patients, and new-onset atrial fibrillation was found in 365 (5.8%). Reperfusion was successfully accomplished in both groups with no difference regarding type of reperfusion. In group 2, therapy with beta-blockers and angiotensin-conversion enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs) was less frequent, 20.6% received anticoagulation at discharge and 16.1% were on triple therapy. New-onset atrial fibrillation was associated with more in-hospital complications and mortality. However, it was not found as an independent predictor of in-hospital mortality. We identified age, prior stroke, inferior myocardial infarction and complete atrioventricular block as independent predictors of new-onset atrial fibrillation.
New-onset atrial fibrillation remains a frequent complication of myocardial infarction and is associated with higher rate of complications and in-hospital mortality. Age, prior stroke, inferior myocardial infarction and complete atrioventricular block were independent predictors of new onset atrial fibrillation. Only 36.7% of the patients received anticoagulation at discharge.
新发心房颤动是急性心肌梗死的一个重要并发症,具有预后意义。
研究 ST 段抬高型心肌梗死住院期间新发心房颤动的发生率、对治疗的影响和死亡率,并确定其发生的预测因素。
我们研究了 2010 年至 2017 年期间连续纳入的葡萄牙国家注册中心的所有 ST 段抬高型心肌梗死患者,并将两组进行比较:1-无心房颤动,2-新发心房颤动。我们调整了逻辑回归模型数据分析,以评估新发心房颤动对住院死亡率的影响,并确定其发生的独立预测因素。p 值<0.05 被认为具有统计学意义。
我们研究了 6325 例患者,其中 365 例(5.8%)发现新发心房颤动。两组的再灌注均成功完成,再灌注类型无差异。在第 2 组中,β受体阻滞剂和血管紧张素转换酶(ACE)抑制剂/血管紧张素受体阻滞剂(ARB)的治疗较少,20.6%的患者在出院时接受抗凝治疗,16.1%的患者接受三联治疗。新发心房颤动与更多的院内并发症和死亡率相关。然而,它并不是住院死亡率的独立预测因素。我们发现年龄、既往卒中、下壁心肌梗死和完全性房室传导阻滞是新发心房颤动的独立预测因素。
新发心房颤动仍然是心肌梗死的常见并发症,与更高的并发症发生率和住院死亡率相关。年龄、既往卒中、下壁心肌梗死和完全性房室传导阻滞是新发心房颤动的独立预测因素。只有 36.7%的患者在出院时接受抗凝治疗。