Moss Travis J, Calland James Forrest, Enfield Kyle B, Gomez-Manjarres Diana C, Ruminski Caroline, DiMarco John P, Lake Douglas E, Moorman J Randall
1Division of Cardiovascular Medicine, Department of Medicine, University of Virginia Health System, Charlottesville, VA. 2Department of Surgery, University of Virginia Health System, Charlottesville, VA. 3Division of Pulmonary and Critical Care Medicine, Department of Medicine, University of Virginia Health System, Charlottesville, VA. 4University of Virginia School of Medicine, Charlottesville, VA.
Crit Care Med. 2017 May;45(5):790-797. doi: 10.1097/CCM.0000000000002325.
To determine the association of new-onset atrial fibrillation with outcomes, including ICU length of stay and survival.
Retrospective cohort of ICU admissions. We found atrial fibrillation using automated detection (≥ 90 s in 30 min) and classed as new-onset if there was no prior diagnosis of atrial fibrillation. We identified determinants of new-onset atrial fibrillation and, using propensity matching, characterized its impact on outcomes.
Tertiary care academic center.
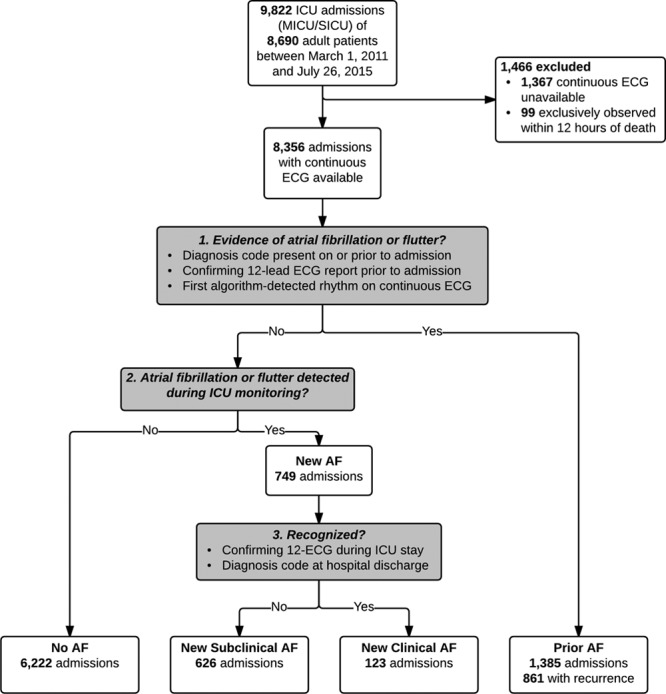
A total of 8,356 consecutive adult admissions to either the medical or surgical/trauma/burn ICU with available continuous electrocardiogram data.
None.
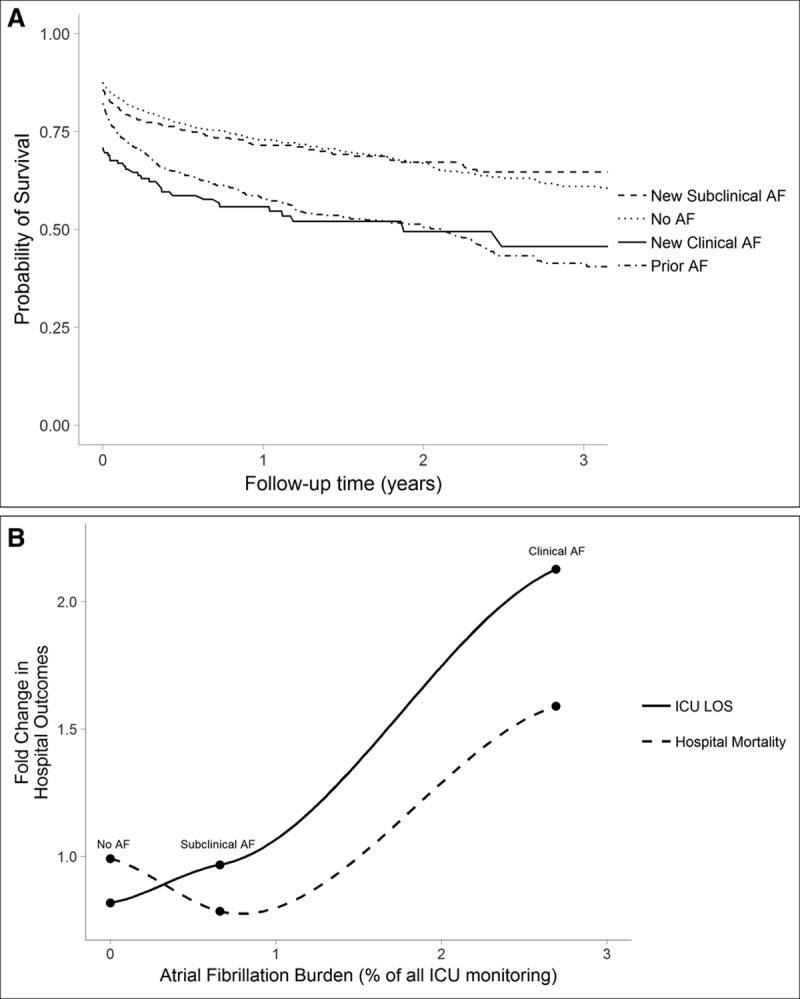
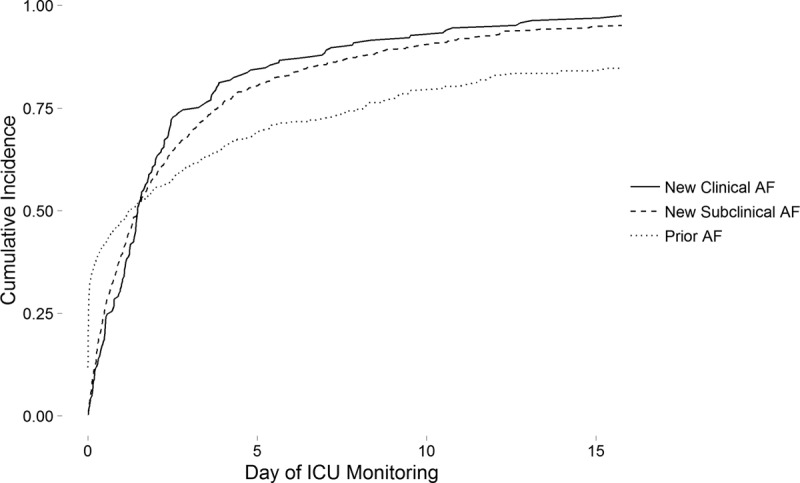
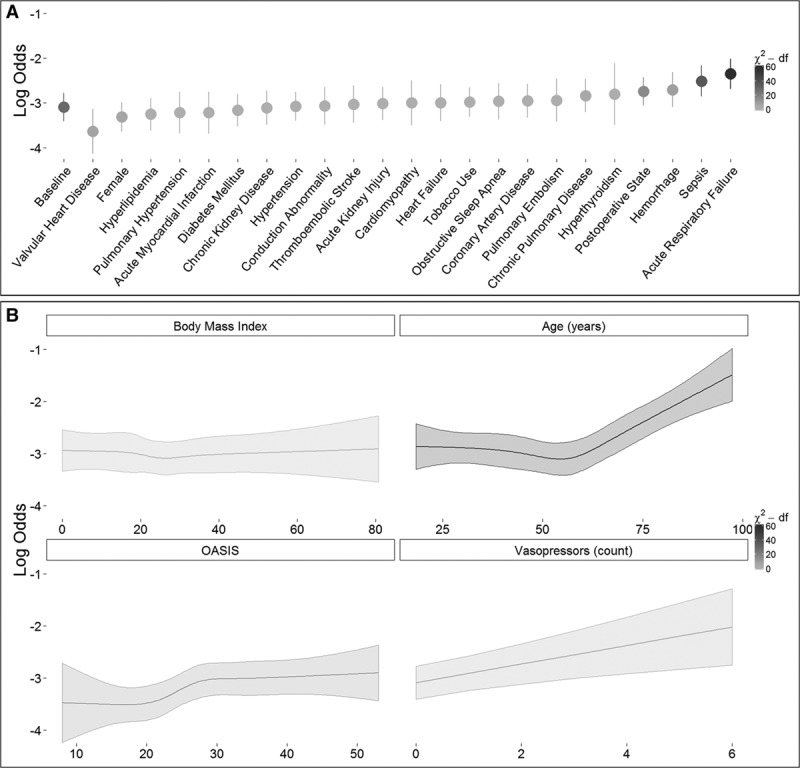
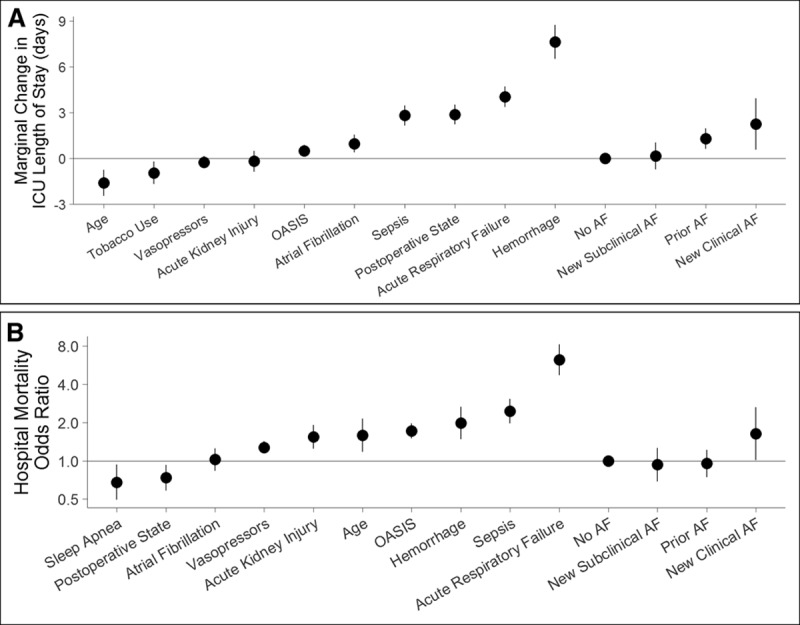
From 74 patient-years of every 15-minute observations, we detected atrial fibrillation in 1,610 admissions (19%), with median burden less than 2%. Most atrial fibrillation was paroxysmal; less than 2% of admissions were always in atrial fibrillation. New-onset atrial fibrillation was subclinical or went undocumented in 626, or 8% of all ICU admissions. Advanced age, acute respiratory failure, and sepsis were the strongest predictors of new-onset atrial fibrillation. In propensity-adjusted regression analyses, clinical new-onset atrial fibrillation was associated with increased hospital mortality (odds ratio, 1.63; 95% CI, 1.01-2.63) and longer length of stay (2.25 d; CI, 0.58-3.92). New-onset atrial fibrillation was not associated with survival after hospital discharge (hazard ratio, 0.99; 95% CI, 0.76-1.28 and hazard ratio, 1.11; 95% CI, 0.67-1.83, respectively, for subclinical and clinical new-onset atrial fibrillation).
Automated analysis of continuous electrocardiogram heart rate dynamics detects new-onset atrial fibrillation in many ICU patients. Though often transient and frequently unrecognized, new-onset atrial fibrillation is associated with poor hospital outcomes.
确定新发房颤与包括重症监护病房(ICU)住院时间和生存率在内的预后之间的关联。
ICU入院患者的回顾性队列研究。我们使用自动检测(30分钟内≥90秒)来发现房颤,若此前未诊断出房颤,则将其归类为新发房颤。我们确定了新发房颤的决定因素,并通过倾向匹配法来描述其对预后的影响。
三级医疗学术中心。
共有8356例连续入住内科或外科/创伤/烧伤ICU且有可用连续心电图数据的成年患者。
无。
在每15分钟观察一次的74个患者年中,我们在1610例入院患者(19%)中检测到房颤,房颤负担中位数小于2%。大多数房颤为阵发性;不到2%的入院患者一直处于房颤状态。626例(占所有ICU入院患者的8%)新发房颤为亚临床型或未被记录。高龄、急性呼吸衰竭和脓毒症是新发房颤的最强预测因素。在倾向调整回归分析中,临床新发房颤与医院死亡率增加(比值比,1.63;95%可信区间,1.01 - 2.63)和住院时间延长(2.25天;可信区间,0.58 - 3.92)相关。新发房颤与出院后生存率无关(风险比,0.99;95%可信区间,0.76 - 1.28,亚临床和临床新发房颤的风险比分别为1.11;95%可信区间,0.67 - 1.83)。
对连续心电图心率动态进行自动分析可在许多ICU患者中检测到新发房颤。尽管新发房颤通常是短暂的且常未被识别,但它与不良的医院预后相关。