Duan Jun, Wang Shengyu, Liu Ping, Han Xiaoli, Tian Yao, Gao Fan, Zhou Jing, Mou Junhuan, Qin Qian, Yu Jingrong, Bai Linfu, Zhou Lintong, Zhang Rui
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, Youyi Road 1, Yuzhong District, Chongqing, 400016, People's Republic of China.
Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Xi'an Medical University, Xi'an, 710077, People's Republic of China.
Ann Intensive Care. 2019 Sep 30;9(1):108. doi: 10.1186/s13613-019-0585-9.
Early identification of noninvasive ventilation (NIV) failure is a promising strategy for reducing mortality in chronic obstructive pulmonary disease (COPD) patients. However, a risk-scoring system is lacking.
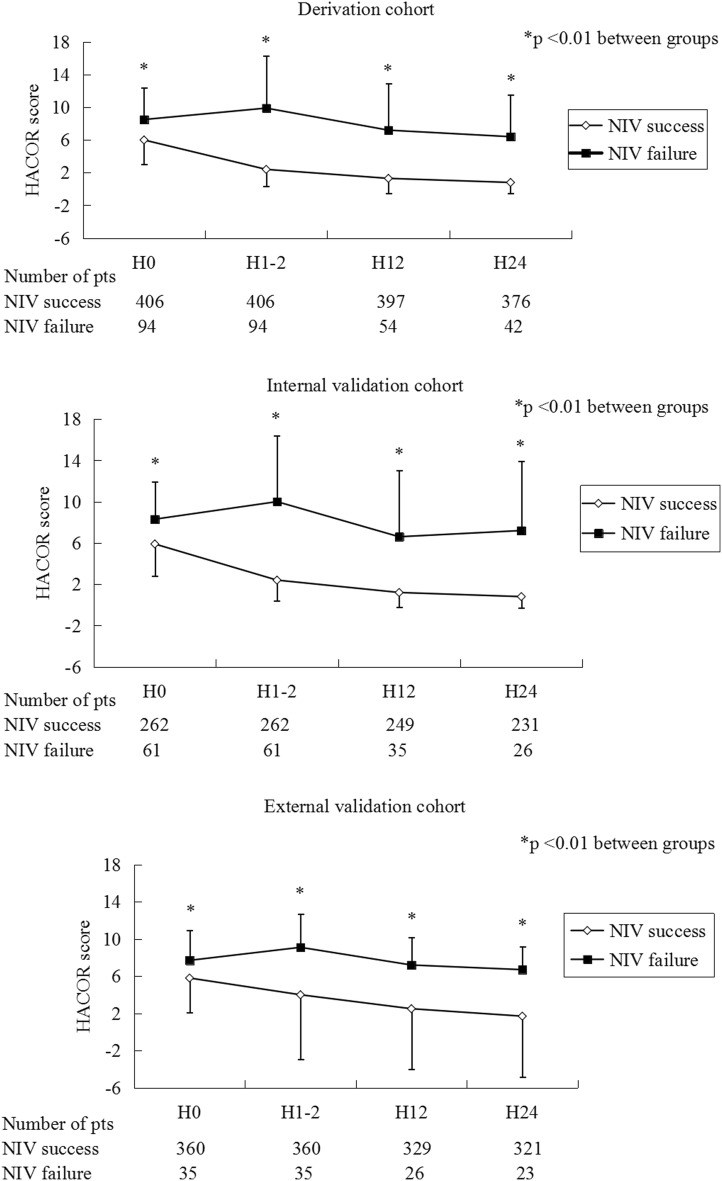
To develop a scale to predict NIV failure, 500 COPD patients were enrolled in a derivation cohort. Heart rate, acidosis (assessed by pH), consciousness (assessed by Glasgow coma score), oxygenation, and respiratory rate (HACOR) were entered into the scoring system. Another two groups of 323 and 395 patients were enrolled to internally and externally validate the scale, respectively. NIV failure was defined as intubation or death during NIV.
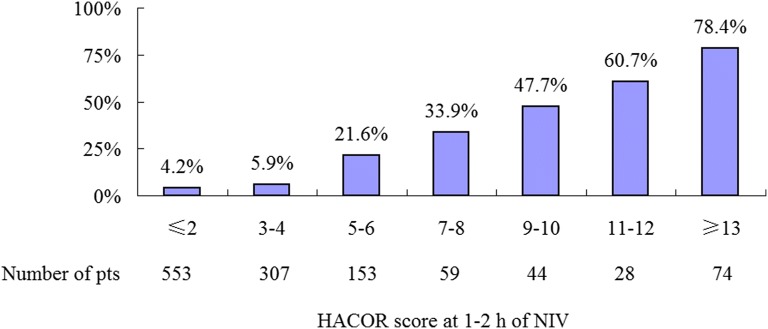
Using HACOR score collected at 1-2 h of NIV to predict NIV failure, the area under the receiver operating characteristic curves (AUC) was 0.90, 0.89, and 0.71 for the derivation, internal-validation, and external-validation cohorts, respectively. For the prediction of early NIV failure in these three cohorts, the AUC was 0.91, 0.96, and 0.83, respectively. In all patients with HACOR score > 5, the NIV failure rate was 50.2%. In these patients, early intubation (< 48 h) was associated with decreased hospital mortality (unadjusted odds ratio = 0.15, 95% confidence interval 0.05-0.39, p < 0.01).
HACOR scores exhibited good predictive power for NIV failure in COPD patients, particularly for the prediction of early NIV failure (< 48 h). In high-risk patients, early intubation was associated with decreased hospital mortality.
早期识别无创通气(NIV)失败是降低慢性阻塞性肺疾病(COPD)患者死亡率的一项有前景的策略。然而,目前缺乏风险评分系统。
为制定一个预测NIV失败的量表,500例COPD患者被纳入推导队列。将心率、酸中毒(通过pH值评估)、意识(通过格拉斯哥昏迷评分评估)、氧合和呼吸频率(HACOR)纳入评分系统。另外两组分别为323例和395例患者,用于对该量表进行内部和外部验证。NIV失败定义为NIV期间插管或死亡。
使用NIV 1 - 2小时时收集的HACOR评分预测NIV失败,推导队列、内部验证队列和外部验证队列的受试者工作特征曲线下面积(AUC)分别为0.90、0.89和0.71。对于这三个队列中早期NIV失败的预测,AUC分别为0.91、0.96和0.83。在所有HACOR评分>5的患者中,NIV失败率为50.2%。在这些患者中,早期插管(<48小时)与医院死亡率降低相关(未调整优势比=0.15,95%置信区间0.05 - 0.39,p<0.01)。
HACOR评分对COPD患者的NIV失败具有良好的预测能力,尤其是对早期NIV失败(<48小时)的预测。在高危患者中,早期插管与医院死亡率降低相关。