Sandra Rotman Centre for Global Health, University Health Network-University of Toronto, Toronto, Ontario, Canada.
College of Medicine, University of Malawi, Blantyre, Malawi.
PLoS Med. 2019 Oct 1;16(10):e1002914. doi: 10.1371/journal.pmed.1002914. eCollection 2019 Oct.
Malaria in pregnancy is associated with adverse birth outcomes. However, the underlying mechanisms remain poorly understood. Tight regulation of angiogenic, metabolic, and inflammatory pathways are essential for healthy pregnancies. We hypothesized that malaria disrupts these pathways leading to preterm birth (PTB).
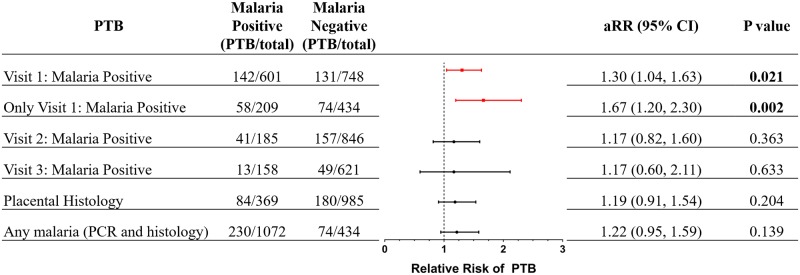
We conducted a secondary analysis of a randomized trial of malaria prevention in pregnancy conducted in Malawi from July 21, 2011, to March 18, 2013. We longitudinally assessed circulating mediators of angiogenic, metabolic, and inflammatory pathways during pregnancy in a cohort of HIV-negative women (n = 1,628), with a median age of 21 years [18, 25], and 562 (35%) were primigravid. Pregnancies were ultrasound dated, and samples were analyzed at 13 to 23 weeks (Visit 1), 28 to 33 weeks (Visit 2), and/or 34 to 36 weeks (Visit 3). Malaria prevalence was high; 70% (n = 1,138) had PCR-positive Plasmodium falciparum infection at least once over the course of pregnancy and/or positive placental histology. The risk of delivering preterm in the entire cohort was 20% (n = 304/1506). Women with malaria before 24 weeks gestation had a higher risk of PTB (24% versus 18%, p = 0.005; adjusted relative risk [aRR] 1.30, 95% confidence interval [CI] 1.04-1.63, p = 0.021); and those who were malaria positive only before week 24 had an even greater risk of PTB (28% versus 17%, p = 0.02; with an aRR of 1.67, 95% CI 1.20-2.30, p = 0.002). Using linear mixed-effects modeling, malaria before 24 weeks gestation was associated with altered kinetics of inflammatory (C-Reactive Protein [CRP], Chitinase 3-like protein-1 [CHI3L1], Interleukin 18 Binding Protein [IL-18BP], soluble Tumor Necrosis Factor receptor II [sTNFRII], soluble Intercellular Adhesion Molecule-1 [sICAM-1]), angiogenic (soluble Endoglin [sEng]), and metabolic mediators (Leptin, Angiopoietin-like 3 [Angptl3]) over the course of pregnancy (χ2 > 13.0, p ≤ 0.001 for each). Limitations include being underpowered to assess the impact on nonviable births, being unable to assess women who had not received any antimalarials, and, because of the exposure to antimalarials in the second trimester, there were limited numbers of malaria infections late in pregnancy.
Current interventions for the prevention of malaria in pregnancy are initiated at the first antenatal visit, usually in the second trimester. In this study, we found that many women are already malaria-infected by their first visit. Malaria infection before 24 weeks gestation was associated with dysregulation of essential regulators of angiogenesis, metabolism, and inflammation and an increased risk of PTB. Preventing malaria earlier in pregnancy may reduce placental dysfunction and thereby improve birth outcomes in malaria-endemic settings.
妊娠疟疾与不良出生结局相关。然而,其潜在机制仍知之甚少。血管生成、代谢和炎症途径的严格调控对健康妊娠至关重要。我们假设疟疾会破坏这些途径,导致早产(PTB)。
我们对 2011 年 7 月 21 日至 2013 年 3 月 18 日期间在马拉维进行的一项妊娠疟疾预防随机试验进行了二次分析。我们对 HIV 阴性女性队列(n=1628)的妊娠期间血管生成、代谢和炎症途径的循环介质进行了纵向评估,中位年龄为 21 岁[18,25],其中 562 人(35%)为初产妇。妊娠通过超声确定,在 13 至 23 周(第 1 次就诊)、28 至 33 周(第 2 次就诊)和/或 34 至 36 周(第 3 次就诊)时分析样本。疟疾流行率很高;70%(n=1138)在妊娠期间至少有一次 PCR 阳性疟原虫感染和/或胎盘组织学阳性。整个队列的早产风险为 20%(n=304/1506)。妊娠 24 周前患有疟疾的女性发生 PTB 的风险更高(24%比 18%,p=0.005;调整后的相对风险[aRR]为 1.30,95%置信区间[CI]为 1.04-1.63,p=0.021);而仅在妊娠 24 周前疟疾阳性的女性发生 PTB 的风险更高(28%比 17%,p=0.02;aRR 为 1.67,95%CI 为 1.20-2.30,p=0.002)。使用线性混合效应模型,妊娠 24 周前的疟疾与炎症(C 反应蛋白[CRP]、几丁质酶 3 样蛋白 1[CHI3L1]、白细胞介素 18 结合蛋白[IL-18BP]、可溶性肿瘤坏死因子受体 II[sTNFRII]、可溶性细胞间黏附分子 1[sICAM-1])、血管生成(可溶性内皮蛋白[sEng])和代谢介质(瘦素、血管生成素样 3[Angptl3])的动力学改变相关(χ2 > 13.0,p ≤ 0.001 每个)。局限性包括评估对不可存活分娩的影响的能力不足、无法评估未接受任何抗疟药物的女性,并且由于在妊娠中期接触抗疟药物,妊娠晚期的疟疾感染数量有限。
目前预防妊娠疟疾的干预措施在第一次产前检查时开始,通常在妊娠中期。在这项研究中,我们发现许多女性在第一次就诊时已经感染了疟疾。妊娠 24 周前的疟疾感染与血管生成、代谢和炎症的重要调节因子失调以及早产风险增加相关。在妊娠早期预防疟疾可能会减少胎盘功能障碍,从而改善疟疾流行地区的出生结局。