Clinic Pasteur of Toulouse Toulouse France.
St. Bartholomew's Hospital Barts Health NHS Trust London United Kingdom.
J Am Heart Assoc. 2019 Oct 15;8(20):e012253. doi: 10.1161/JAHA.119.012253. Epub 2019 Oct 4.
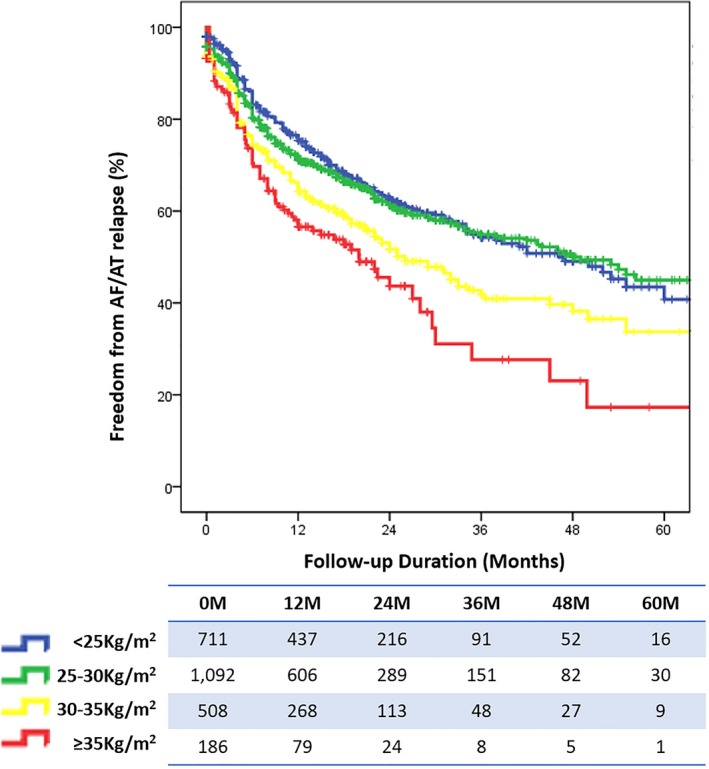
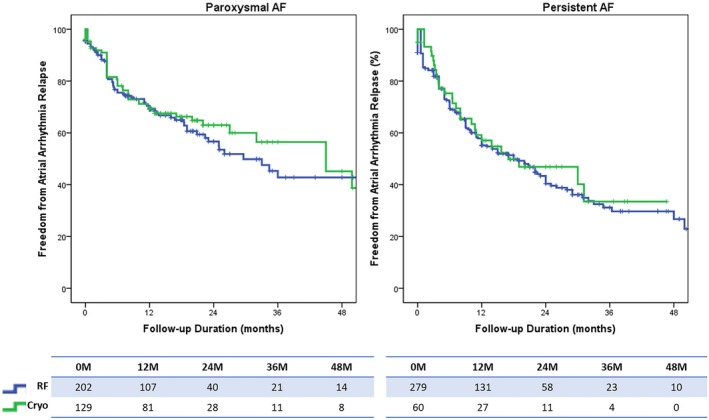
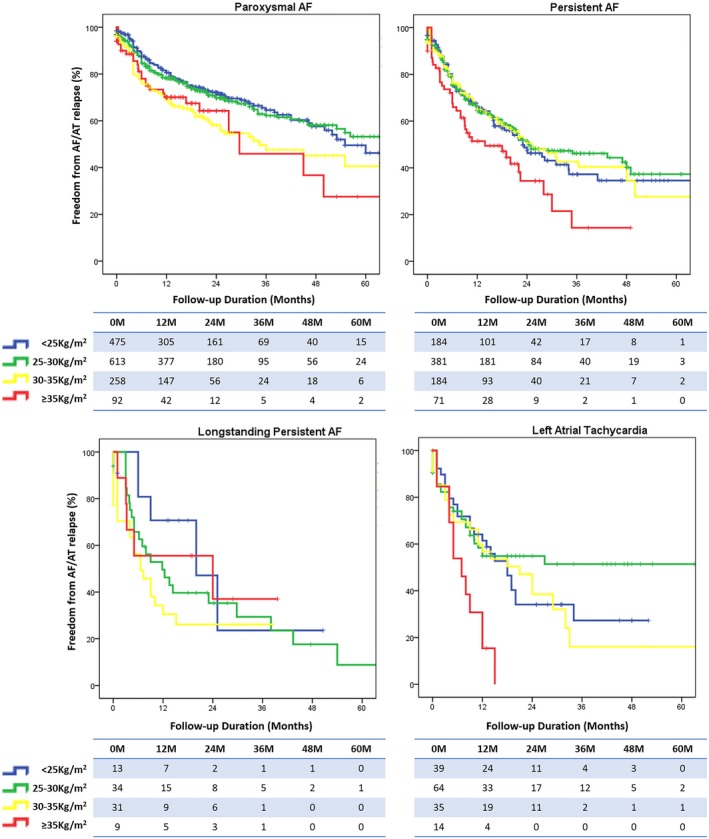
Background Outcomes of catheter ablation of atrial fibrillation (AF) are variable and the predictors of success require further elucidation since the identification of correctable risk factors could help to optimize therapy. We aimed to assess the impact of body mass index (BMI) in the overall safety and efficacy of catheter ablation of AF, with emphasis on the use of cryoballoon ablation and novel oral anticoagulants. Methods and Results There were 2497 consecutive patients undergoing catheter ablation of AF in 7 European high volume centers were stratified according to BMI (normal weight <25 kg/m, pre-obese 25-30 kg/m, obesity 30-35 kg/m, and morbid obesity ≥35 kg/m) and comparisons of procedural outcomes evaluated. Pre-obese and obese patients presented more comorbidities (hypertension, diabetes mellitus, and sleep apnea), and had higher rates of non-paroxysmal AF ablation procedures. The rate of atrial 12-month arrhythmia relapse increased alongside with BMI (35.2%, 35.7%, 43.6%, and 48.0% <0.001). During a median follow-up of 18.8 months (interquartile range 11-28), after adjusting for all baseline differences, BMI was an independent predictor of relapse (hazard ratio=1.01 per kg/m; 95% CI 1.01-1.02; =0.002), adding incremental predictive value to obstructive sleep apnea. BMI was not a predictor for any of the reported complications. Using novel oral anticoagulants and cryoballoon ablation was safe and efficacy was comparable with vitamin-K antagonists and radiofrequency ablation. Conclusions Obese patients present with a more adverse comorbidity profile, more advanced forms of AF, and have lower chances of being free from AF relapse after ablation. Use of novel oral anticoagulants and cryoballoon ablation may be an option in this patient group.
背景 房颤(AF)导管消融的结果各不相同,成功的预测因素仍需进一步阐明,因为确定可纠正的危险因素有助于优化治疗。我们旨在评估体重指数(BMI)对 AF 导管消融整体安全性和有效性的影响,重点关注冷冻球囊消融和新型口服抗凝剂的应用。
方法和结果 在 7 个欧洲大容量中心,共有 2497 例连续接受 AF 导管消融的患者根据 BMI(正常体重<25kg/m²,超重 25-30kg/m²,肥胖 30-35kg/m²,病态肥胖≥35kg/m²)进行分层,并评估了手术结果的比较。超重和肥胖患者存在更多的合并症(高血压、糖尿病和睡眠呼吸暂停),非阵发性 AF 消融的比例更高。12 个月时心房心律失常复发率随 BMI 增加而增加(35.2%、35.7%、43.6%和 48.0%<0.001)。在中位数为 18.8 个月(四分位距 11-28)的随访期间,在调整所有基线差异后,BMI 是复发的独立预测因素(风险比=每公斤 1.01;95%置信区间 1.01-1.02;=0.002),对阻塞性睡眠呼吸暂停有额外的预测价值。BMI 不是任何报告的并发症的预测因素。使用新型口服抗凝剂和冷冻球囊消融是安全的,其疗效与维生素 K 拮抗剂和射频消融相当。
结论 肥胖患者具有更不利的合并症谱、更晚期的 AF 形式,消融后 AF 复发的几率更低。在该患者群体中,使用新型口服抗凝剂和冷冻球囊消融可能是一种选择。