Departments of Cardiothoracic Surgery (A.B.G., P.C., B.L., M.P.F., Y.J.W.), Department of Medicine, Stanford University, CA.
Health Research and Policy (A.B.G., P.C.), Department of Medicine, Stanford University, CA.
Circulation. 2019 Oct 8;140(15):1239-1250. doi: 10.1161/CIRCULATIONAHA.118.038867. Epub 2019 Oct 7.
The feasibility and effectiveness of delaying surgery to transfer patients with acute type A aortic dissection-a catastrophic disease that requires prompt intervention-to higher-volume aortic surgery hospitals is unknown. We investigated the hypothesis that regionalizing care at high-volume hospitals for acute type A aortic dissections will lower mortality. We further decomposed this hypothesis into subparts, investigating the isolated effect of transfer and the isolated effect of receiving care at a high-volume versus a low-volume facility.
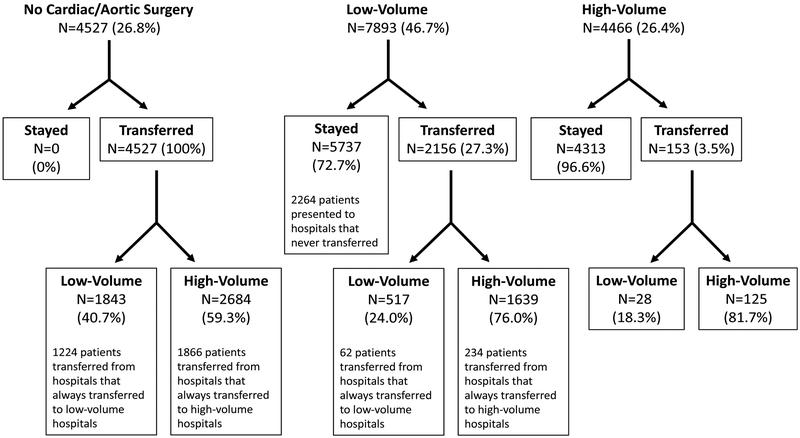
We compared the operative mortality and long-term survival between 16 886 Medicare beneficiaries diagnosed with an acute type A aortic dissection between 1999 and 2014 who (1) were transferred versus not transferred, (2) underwent surgery at high-volume versus low-volume hospitals, and (3) were rerouted versus not rerouted to a high-volume hospital for treatment. We used a preference-based instrumental variable design to address unmeasured confounding and matching to separate the effect of transfer from volume.
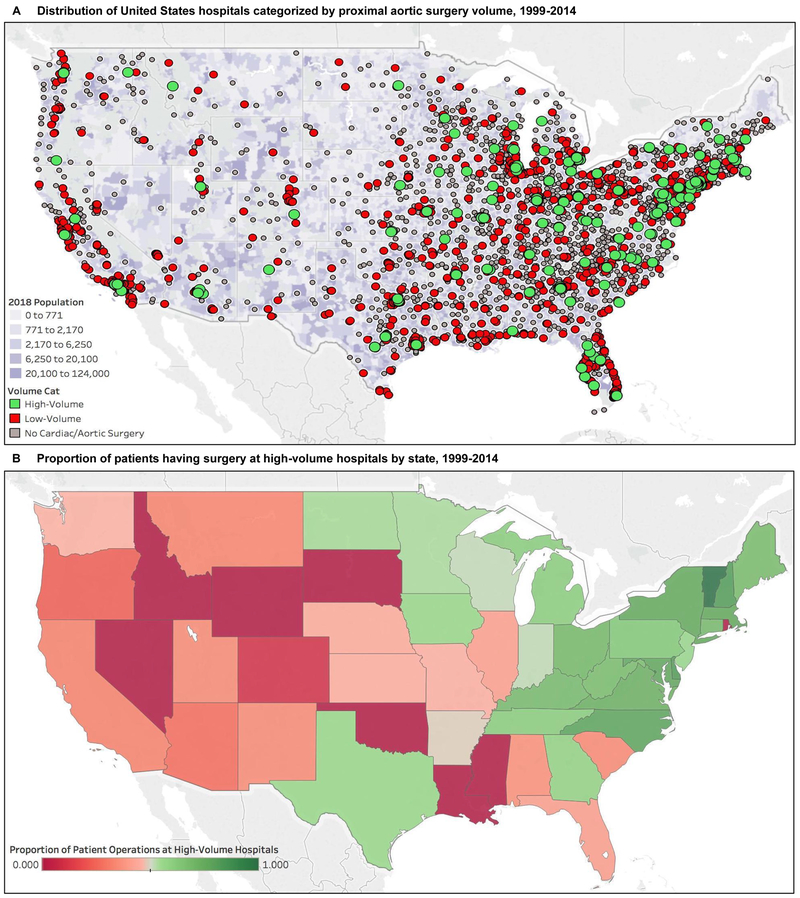
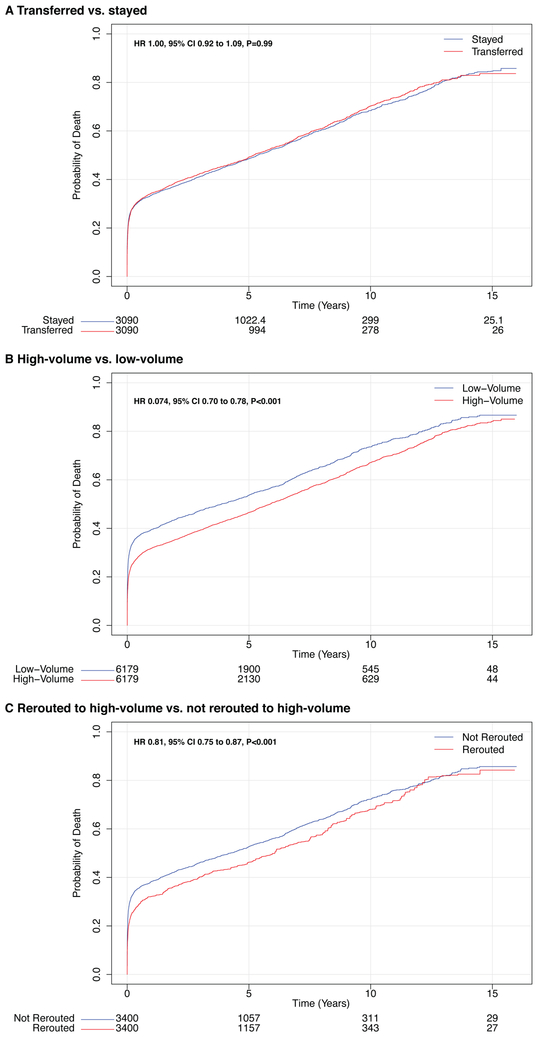
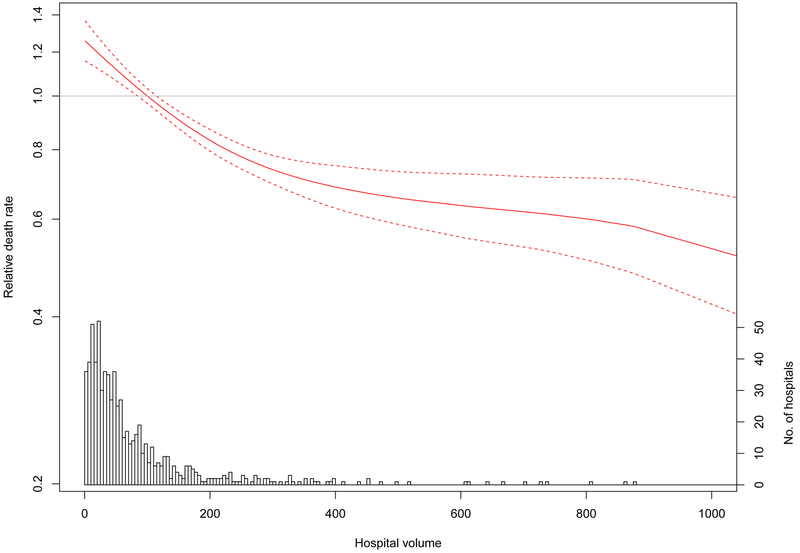
Between 1999 and 2014, 40.5% of patients with an acute type A aortic dissection were transferred, and 51.9% received surgery at a high-volume hospital. Interfacility transfer was not associated with a change in operative mortality (risk difference, -0.69%; 95% CI, -2.7% to 1.35%) or long-term mortality. Despite delaying surgery, a regionalization policy that transfers patients to high-volume hospitals was associated with a 7.2% (95% CI, 4.1%-10.3%) absolute risk reduction in operative mortality; this association persisted in the long term (hazard ratio, 0.81; 95% CI, 0.75-0.87). The median distance needed to reroute each patient to a high-volume hospital was 50.1 miles (interquartile range, 12.4-105.4 miles).
Operative and long-term mortality were substantially reduced in patients with acute type A aortic dissection who were rerouted to high-volume hospitals. Policy makers should evaluate the feasibility and benefits of regionalizing the surgical treatment of acute type A aortic dissection in the United States.
将急性 A 型主动脉夹层(一种需要立即介入治疗的灾难性疾病)患者延迟手术转移至大容量主动脉手术医院的可行性和效果尚不清楚。我们研究了这样一个假设,即在大容量医院对急性 A 型主动脉夹层进行区域化治疗将降低死亡率。我们进一步将这一假设分解为几个部分,分别研究转院和在大容量与小容量医院接受治疗的单独效果。
我们比较了 1999 年至 2014 年间,16886 名被诊断为急性 A 型主动脉夹层的 Medicare 受益人的手术死亡率和长期生存率,这些患者(1)是否转院,(2)在大容量医院还是小容量医院接受手术,(3)是否转至大容量医院治疗。我们使用基于偏好的工具变量设计来解决未测量的混杂因素,并通过匹配来分离转院和容量的影响。
1999 年至 2014 年间,40.5%的急性 A 型主动脉夹层患者转院,51.9%的患者在大容量医院接受手术。医院间转院与手术死亡率无变化相关(风险差异,-0.69%;95%CI,-2.7%至 1.35%)或长期死亡率。尽管延迟了手术,但将患者转至大容量医院的区域化政策与手术死亡率降低 7.2%(95%CI,4.1%-10.3%)相关;这一关联在长期内仍然存在(风险比,0.81;95%CI,0.75-0.87)。为了将每个患者转至大容量医院,所需的平均距离为 50.1 英里(中位数,12.4-105.4 英里)。
转至大容量医院的急性 A 型主动脉夹层患者的手术和长期死亡率显著降低。政策制定者应评估在美国对急性 A 型主动脉夹层进行手术治疗的区域化的可行性和益处。