Department of Radiation Oncology, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT, USA.
Division of Epidemiology, School of Medicine, University of Utah, Salt Lake City, UT, USA.
Lung Cancer. 2019 Dec;138:6-12. doi: 10.1016/j.lungcan.2019.09.009. Epub 2019 Sep 16.
To compare patterns of care and overall survival (OS) between stereotactic body radiotherapy (SBRT) and percutaneous local tumor ablation (LTA) for non-surgically managed early-stage non-small-cell lung cancer (NSCLC).
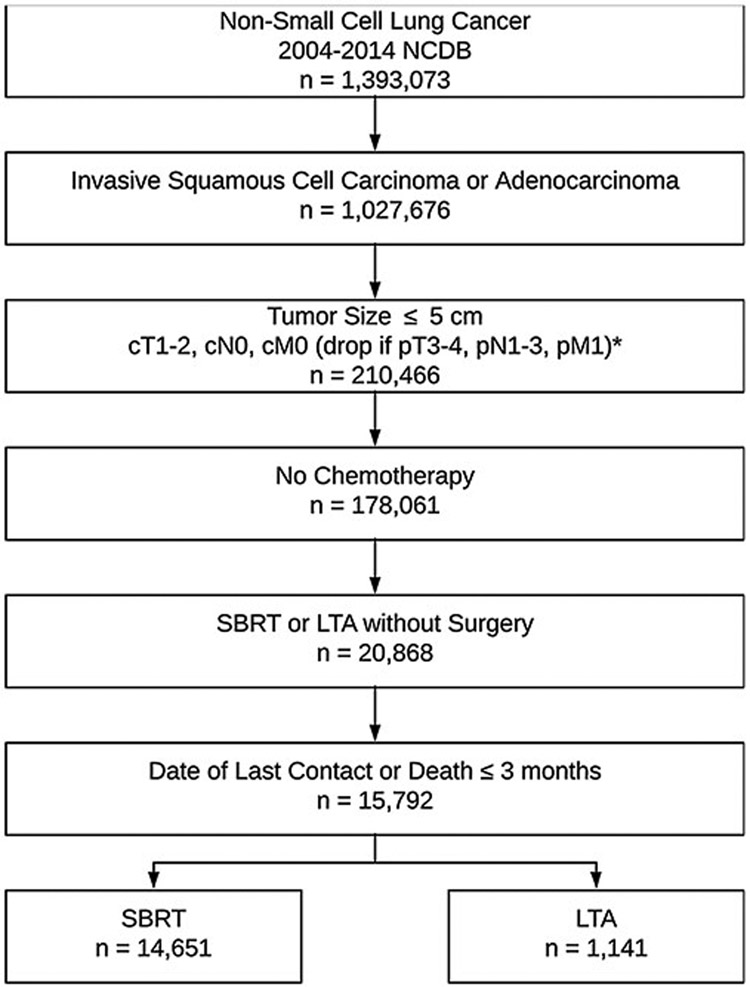
The National Cancer Database (NCDB) was queried from 2004 to 2014 for adults with non-metastatic, node-negative invasive adenocarcinoma or squamous cell carcinoma of the lung with primary tumor size ≤5.0 cm who did not undergo surgery or chemotherapy and received SBRT or LTA. Patterns of care were assessed with multivariate logistic regression. After propensity-score weighting with generalized boosted regression, OS was assessed with univariate and doubly-robust multivariate Cox regression.
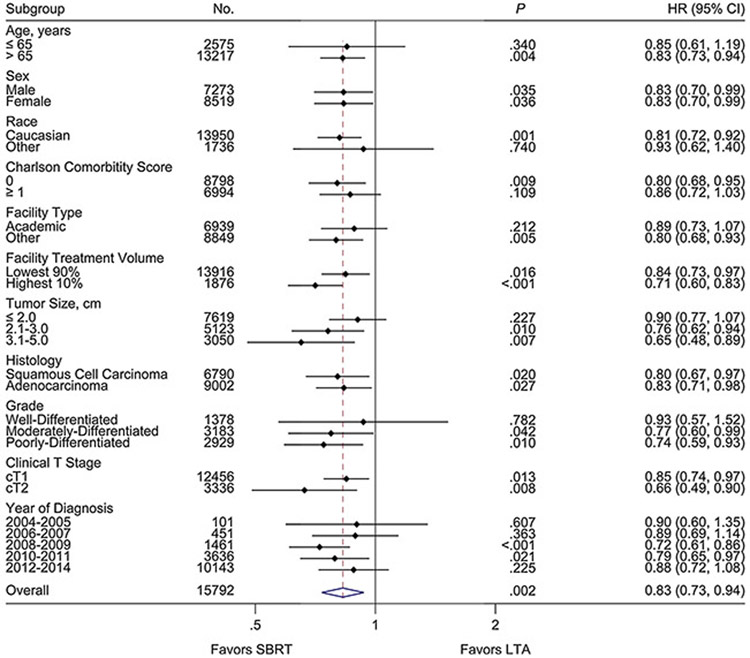
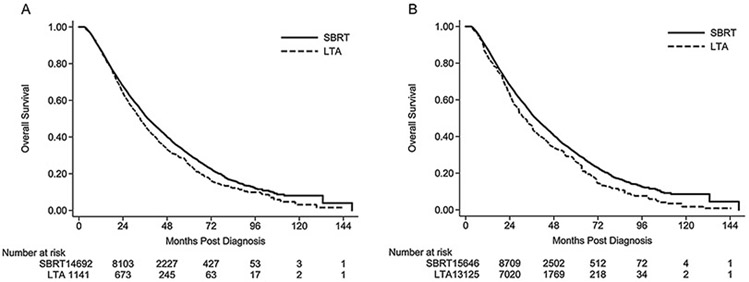
Of 15,792 patients, 14,651 (93%) received SBRT and 1141 (7%) received LTA. Increasing age (OR 1.01, p = .035), treatment at an academic institution (OR 2.94, p < .001), increasing tumor size (OR 1.05, p < .001), and more recent year of diagnosis (OR 1.43, p < .001) were predictive of treatment with SBRT, whereas comorbidities (OR 0.74, p = .003) and treatment at a high-volume facility (OR 0.05, p < .001) were predictive for LTA. At a median follow-up of 26.2 months, SBRT was associated with improved OS relative to LTA within a propensity-score weighted doubly-robust multivariate analysis (HR 0.71, p < .001). On weighted subgroup analyses, improved OS was observed with SBRT for tumor sizes >2.0 cm (HR 0.72, p < .001) and for those treated at high-volume facilities (HR 0.71, p < .001). No OS difference was found with SBRT or LTA in tumor sizes ≤2.0 cm (HR 0.90, p = .227).
Within the NCDB, SBRT was more commonly utilized and was associated with improved OS when compared to percutaneous LTA for patients with non-surgically managed early-stage NSCLC. Patients with small tumor volumes likely represent an appropriate population for future prospective randomized comparisons between SBRT and LTA.
比较立体定向体部放射治疗(SBRT)和经皮局部肿瘤消融(LTA)治疗非手术管理的早期非小细胞肺癌(NSCLC)的治疗模式和总生存率(OS)。
从 2004 年至 2014 年,国家癌症数据库(NCDB)对未接受手术或化疗且接受 SBRT 或 LTA 治疗的非转移性、淋巴结阴性、原发性肿瘤大小≤5.0cm 的非小细胞浸润性腺癌或鳞状细胞癌的成年人进行了查询。采用多变量逻辑回归评估治疗模式。在使用广义提升回归进行倾向评分加权后,采用单变量和双重稳健多变量 Cox 回归评估 OS。
在 15792 名患者中,14651 名(93%)接受 SBRT 治疗,1141 名(7%)接受 LTA 治疗。年龄增长(OR 1.01,p=0.035)、在学术机构治疗(OR 2.94,p<0.001)、肿瘤体积增大(OR 1.05,p<0.001)和较晚的诊断年份(OR 1.43,p<0.001)是接受 SBRT 治疗的预测因素,而合并症(OR 0.74,p=0.003)和在大容量设施治疗(OR 0.05,p<0.001)是接受 LTA 治疗的预测因素。在中位随访 26.2 个月后,在倾向评分加权双重稳健多变量分析中,SBRT 与 LTA 相比,OS 得到改善(HR 0.71,p<0.001)。在加权亚组分析中,对于肿瘤大小>2.0cm(HR 0.72,p<0.001)和在大容量设施治疗的患者(HR 0.71,p<0.001),SBRT 可改善 OS。在肿瘤大小≤2.0cm 时,SBRT 或 LTA 治疗与 OS 无差异(HR 0.90,p=0.227)。
在 NCDB 中,与经皮 LTA 相比,SBRT 更常用于治疗非手术管理的早期 NSCLC 患者,并且与 OS 改善相关。对于肿瘤体积较小的患者,SBRT 和 LTA 之间的未来前瞻性随机比较可能是一个合适的研究人群。