Institute of Hospital Management, West China Hospital, Sichuan University, Guo Xue Xiang 37, Chengdu, Sichuan, China.
Department of Anesthesiology, West China Hospital, Sichuan University, Guo Xue Xiang 37, Chengdu, 610041, Sichuan, China.
BMC Anesthesiol. 2019 Oct 9;19(1):178. doi: 10.1186/s12871-019-0852-1.
Increase of pulmonary vascular resistance (PVR) is an efficient method of modulating pulmonary and systemic blood flows (Qp/Qs) for patients with left-to-right (L-R) shunt, and is also closely associated with insufficient oxygen exchange for pulmonary hypoperfusion. So that it might be a preferred regime of maintaining arterial partial pressure of carbon dioxide tension (PaCO) within an optimal boundary via ventilation management in congenital heart disease (CHD) patients for the inconvenient measure of the PVR and Qp/Qs. However, the appropriate range of PaCO and patient-specific mechanical ventilation settings remain controversial for CHD children with L-R shunt.
Thirty-one pediatric patients with L-R shunt, 1-6 yr of age, were included in this observation study. Patients were ventilated with tidal volume (V) of 10, 8 and 6 ml/kg in sequence, and 15 min stabilization period for individual V. The velocity time integral (VTI) of L-R shunt, pulmonary artery (PA) and descending aorta (DA) were measured with transesophageal echocardiography (TEE) after an initial 15 min stabilization period for each V, with arterial blood gas analysis. Near-infrared spectroscopy sensor were positioned on the surface of the bilateral temporal artery to monitor the change in regional cerebral oxygen saturation (rScO).
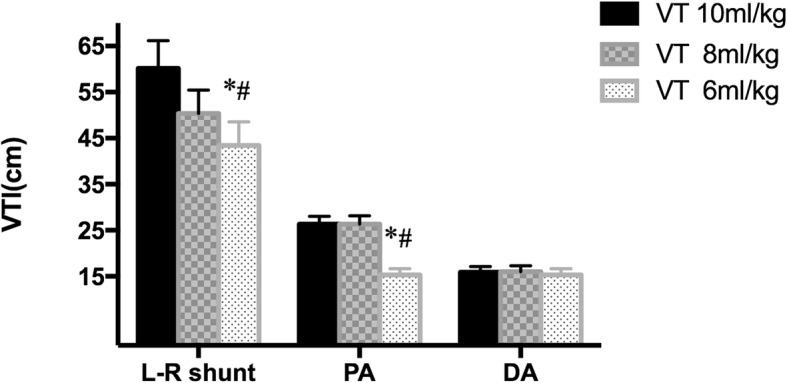
PaCO was 31.51 ± 0.65 mmHg at V 10 ml/kg vs. 37.15 ± 0.75 mmHg at V 8 ml/kg (P < 0.03), with 44.24 ± 0.99 mmHg at V 6 ml/kg significantly higher than 37.15 ± 0.75 mmHg at V 8 ml/kg. However, PaO at a V of 6 ml/kg was lower than that at a V of 10 ml/kg (P = 0.05). Meanwhile, 72% (22/31) patients had PaCO in the range of 40-50 mmHg at V 6 ml/kg. VTI of L-R shunt and PA at V 6 ml/kg were lower than that at V of 8 and 10 ml/kg (P < 0.05). rScO at a V of 6 ml/kg was higher than that at a V of 8 and 10 ml/kg (P < 0.05), with a significantly correlation between rScO and PaCO (r = 0.53). VTI of PA in patients with defect diameter > 10 mm was higher that that in patients with defect diameter ≤ 10 mm.
Maintaining PaCO in the boundary of 40-50 mmHg with V 6 ml/kg might be a feasible ventilation regime to achieve better oxygenation for patients with L-R shunt. Continue raising PaCO should be careful.
Clinical Trial Registry of China (http://www.chictr.org.cn) identifier: ChiCTR-OOC-17011338 , prospectively registered on May 9, 2017.
增加肺血管阻力(PVR)是调节左向右分流(L-R)患者肺和全身血流量(Qp/Qs)的有效方法,也与肺灌注不足导致的氧气交换不足密切相关。因此,对于先天性心脏病(CHD)患者,通过通气管理来维持动脉二氧化碳分压(PaCO)在最佳范围内可能是维持 PaCO 的首选方案,因为不方便测量 PVR 和 Qp/Qs。然而,对于 L-R 分流的 CHD 儿童,合适的 PaCO 范围和患者特定的机械通气设置仍存在争议。
本观察研究纳入了 31 例年龄在 1-6 岁的 L-R 分流患儿。患者依次接受 10、8 和 6ml/kg 的潮气量(V)通气,并对每个 V 进行 15 分钟的稳定期。在每个 V 的初始 15 分钟稳定期后,通过经食管超声心动图(TEE)测量 L-R 分流、肺动脉(PA)和降主动脉(DA)的速度时间积分(VTI),并进行动脉血气分析。近红外光谱传感器放置在双侧颞动脉表面,以监测局部脑氧饱和度(rScO)的变化。
在 V 10ml/kg 时 PaCO 为 31.51±0.65mmHg,在 V 8ml/kg 时为 37.15±0.75mmHg(P<0.03),在 V 6ml/kg 时为 44.24±0.99mmHg,明显高于 V 8ml/kg 时的 37.15±0.75mmHg。然而,在 V 6ml/kg 时 PaO 低于 V 10ml/kg(P=0.05)。同时,在 V 6ml/kg 时,72%(22/31)的患者 PaCO 在 40-50mmHg 范围内。在 V 6ml/kg 时,L-R 分流和 PA 的 VTI 低于 V 8 和 10ml/kg(P<0.05)。在 V 6ml/kg 时 rScO 高于 V 8 和 10ml/kg(P<0.05),rScO 与 PaCO 之间存在显著相关性(r=0.53)。PA 的 VTI 在缺损直径>10mm 的患者中高于缺损直径≤10mm 的患者。
以 6ml/kg 的 V 维持 PaCO 在 40-50mmHg 的边界内可能是 L-R 分流患者实现更好氧合的可行通气方案。继续升高 PaCO 应谨慎。
中国临床试验注册中心(http://www.chictr.org.cn)注册号:ChiCTR-OOC-17011338,于 2017 年 5 月 9 日前瞻性注册。