Infection and Immunity, Murdoch Children's Research Institute, Parkville, Victoria, Australia; Centre for International Child Health, Department of Paediatrics, The University of Melbourne, Parkville, Victoria, Australia.
Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Vaccine. 2020 Jan 10;38(2):202-211. doi: 10.1016/j.vaccine.2019.10.030. Epub 2019 Oct 23.
Pneumococcal carriage is a prerequisite for pneumococcal disease. Little is known about whether social contact frequency and intensity are associated with pneumococcal carriage. In Fiji, indigenous iTaukei have higher prevalence of pneumococcal carriage compared with Fijians of Indian Descent (FID). We hypothesised that contact differences may contribute to ethnic differences in pneumococcal carriage prevalence and density.
In 2015, young infants (5-8 weeks), toddlers (12-23 months), children (2-6 years), and caregivers from Suva and surrounding areas, participated in a cross-sectional survey (n = 2014), three years post pneumococcal conjugate vaccine introduction. Demographic and contact data, and nasopharyngeal swabs were collected. Pneumococci were detected, and quantified using quantitative real-time PCR, with molecular serotyping by microarray. Associations between ethnicity, contact, and pneumococcal carriage and density were estimated using multivariable generalised estimating equation regression models.
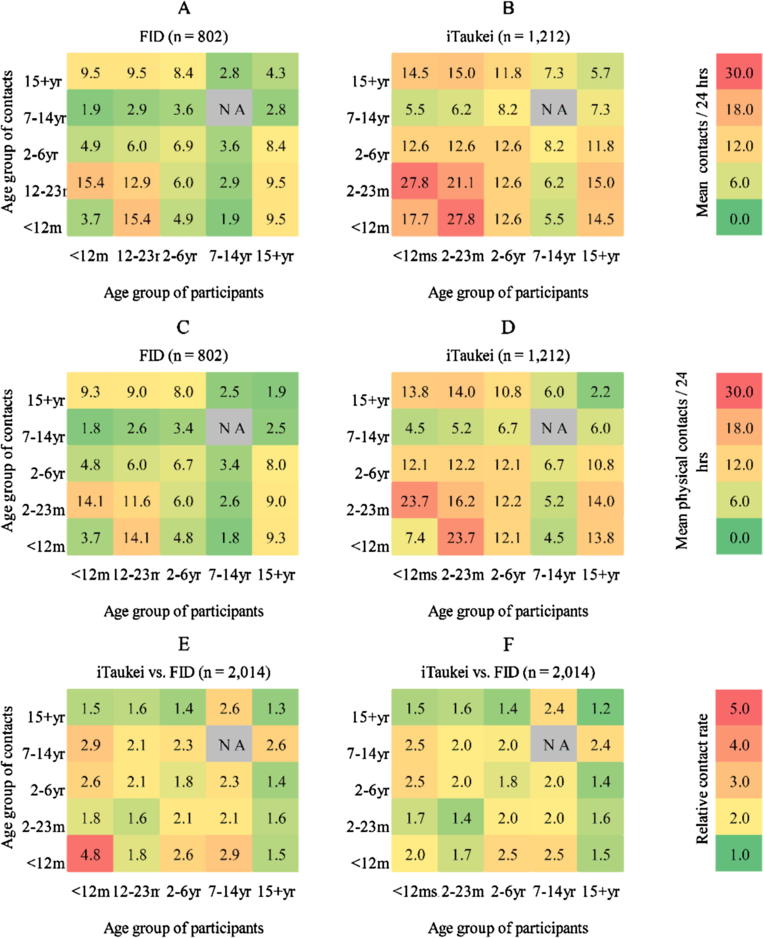
iTaukei participants had larger household sizes, higher pneumococcal carriage rates, more contacts, and more frequent contacts of longer duration, compared with FID. The odds of vaccine-type carriage increased by 28% (95% CI 8-53%) P < 0.01 in association with physical contact with 7-14 year old children. iTaukei ethnicity was associated with vaccine-type carriage (aOR) 1.73; 95% CI 1.06-2.82, P = 0.03) and non-vaccine type carriage (aOR 5.98; 95% CI 4.47-8.00, P < 0.01). Ethnicity and contact were not associated with pneumococcal density.
iTaukei had greater frequency and intensity of contact compared with FID. Physical contact was associated with pneumococcal carriage. Observed differences in pneumococcal nasopharyngeal carriage prevalence between iTaukei and FID were not explained by differences in social contact patterns by ethnicity.
肺炎球菌带菌是肺炎球菌病的前提。目前对于社会接触频率和强度是否与肺炎球菌带菌有关知之甚少。在斐济,土着的伊塔基人比印度裔斐济人(FID)的肺炎球菌带菌率更高。我们假设接触差异可能导致肺炎球菌带菌率和密度的种族差异。
2015 年,5-8 周龄的婴儿、12-23 月龄的幼儿、2-6 岁的儿童及其照顾者来自苏瓦及其周边地区,参与了一项横断面调查(n=2014 人),这是在引入肺炎球菌结合疫苗三年后进行的。收集了人口统计学和接触数据以及鼻咽拭子。使用定量实时 PCR 检测肺炎球菌,并通过微阵列进行分子血清型分型。使用多变量广义估计方程回归模型估计种族、接触和肺炎球菌带菌率和密度之间的关联。
与 FID 相比,伊塔基参与者的家庭规模更大,肺炎球菌带菌率更高,接触更多,接触时间更长且更频繁。与 7-14 岁儿童的身体接触增加了 28%(95%CI 8-53%),疫苗型携带的可能性增加了。与 FID 相比,伊塔基族裔与疫苗型携带(优势比[aOR]1.73;95%CI 1.06-2.82,P=0.03)和非疫苗型携带(aOR 5.98;95%CI 4.47-8.00,P<0.01)有关。种族和接触与肺炎球菌密度无关。
与 FID 相比,伊塔基人的接触频率更高,强度更大。身体接触与肺炎球菌带菌有关。伊塔基人和 FID 之间肺炎球菌鼻咽带菌率的差异不能用种族之间社会接触模式的差异来解释。