Cardiothoracic and Vascular Health Kolling Institute and Department of Cardiology Royal North Shore Hospital Northern Sydney Local Health District St Leonards Australia.
Charles Perkins Centre University of Sydney Australia.
J Am Heart Assoc. 2019 Nov 5;8(21):e013296. doi: 10.1161/JAHA.119.013296. Epub 2019 Nov 1.
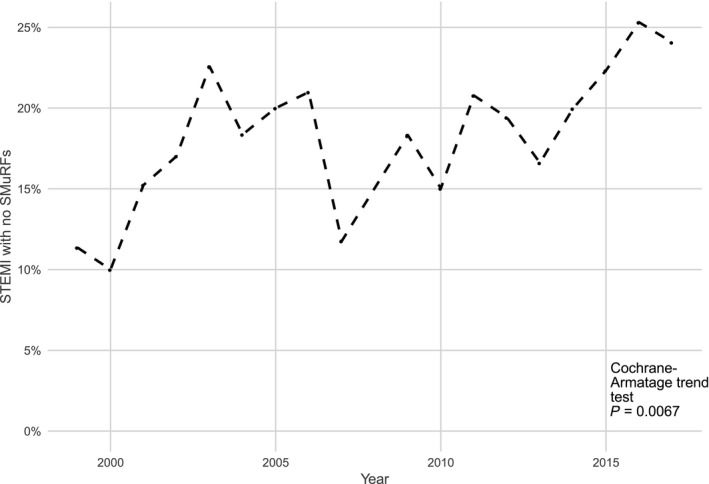
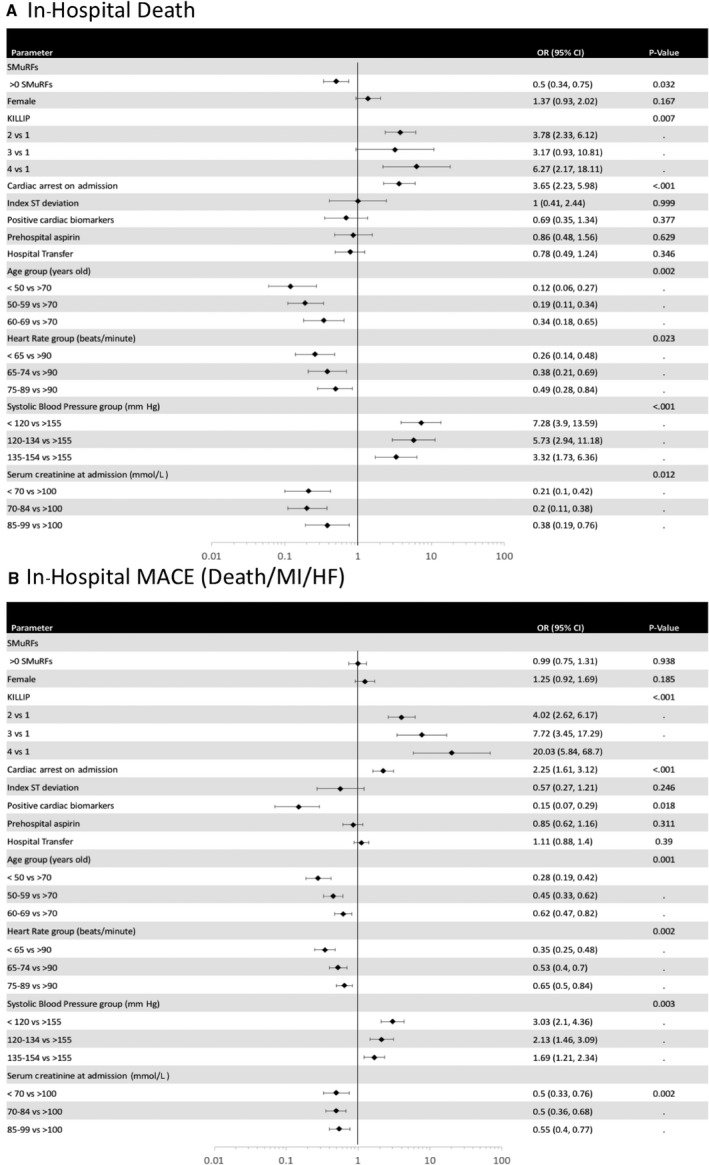
Background Programs targeting the standard modifiable cardiovascular risk factors (SMuRFs: hypertension, diabetes mellitus, hypercholesterolemia, smoking) are critical to tackling coronary heart disease at a community level. However, myocardial infarction in SMuRF-less individuals is not uncommon. This study uses 2 sequential large, multicenter registries to examine the proportion and outcomes of SMuRF-less ST-segment-elevation myocardial infarction (STEMI) patients. Methods and Results We identified 3081 STEMI patients without a prior history of cardiovascular disease in the Australian GRACE (Global Registry of Acute Coronary Events) and CONCORDANCE (Cooperative National Registry of Acute Coronary Syndrome Care) registries, encompassing 42 hospitals, between 1999 and 2017. We examined the proportion that were SMuRF-less as well as outcomes. The primary outcome was in-hospital mortality, and the secondary outcome was major adverse cardiovascular events (death, myocardial infarction, or heart failure, during the index admission). Multivariate regression models were used to identify predictors of major adverse cardiovascular events. Of STEMI patients without a prior history of cardiovascular disease 19% also had no history of SMuRFs. This proportion increased from 14% to 23% during the study period (=0.0067). SMuRF-less individuals had a higher in-hospital mortality rate than individuals with 1 or more SMuRFs. There were no clinically significant differences in major adverse cardiovascular events at 6 months between the 2 groups. Conclusions A substantial and increasing proportion of STEMI presentations occur independently of SMuRFs. Discovery of new markers and mechanisms of disease beyond standard risk factors may facilitate novel preventative strategies. Studies to assess longer-term outcomes of SMuRF-less STEMI patients are warranted.
背景 针对标准可调节心血管风险因素(SMuRFs:高血压、糖尿病、高胆固醇血症、吸烟)的计划对于在社区层面解决冠心病至关重要。然而,SMuRF 缺乏的个体发生心肌梗死并不罕见。本研究使用 2 个连续的大型多中心登记处,检查 SMuRF 缺乏的 ST 段抬高型心肌梗死(STEMI)患者的比例和结局。
方法和结果 我们在澳大利亚 GRACE(全球急性冠状动脉事件登记处)和 CONCORDANCE(急性冠状动脉综合征协同国家登记处)登记处中确定了 3081 例无心血管疾病既往史的 STEMI 患者,该登记处包括 1999 年至 2017 年间的 42 家医院。我们检查了 SMuRF 缺乏的比例以及结局。主要结局是院内死亡率,次要结局是主要不良心血管事件(索引入院期间死亡、心肌梗死或心力衰竭)。使用多变量回归模型确定主要不良心血管事件的预测因素。在无心血管疾病既往史的 STEMI 患者中,有 19%也没有 SMuRFs 既往史。在此期间,这一比例从 14%增加到 23%(=0.0067)。与有 1 种或多种 SMuRFs 的个体相比,SMuRF 缺乏的个体院内死亡率更高。两组在 6 个月时主要不良心血管事件无临床显著差异。
结论 大量且不断增加的 STEMI 发作独立于 SMuRFs 发生。除标准危险因素外,发现新的疾病标志物和机制可能有助于制定新的预防策略。需要评估 SMuRF 缺乏的 STEMI 患者的长期结局的研究。