Department of Pathology, University of Pittsburgh School of Medicine, UPMC Children's Hospital of Pittsburgh, Pittsburgh, PA, USA.
Department of Pathology, University of Utah, Primary Children's Hospital, Salt Lake City, UT, USA.
Acta Neuropathol Commun. 2019 Nov 4;7(1):168. doi: 10.1186/s40478-019-0811-6.
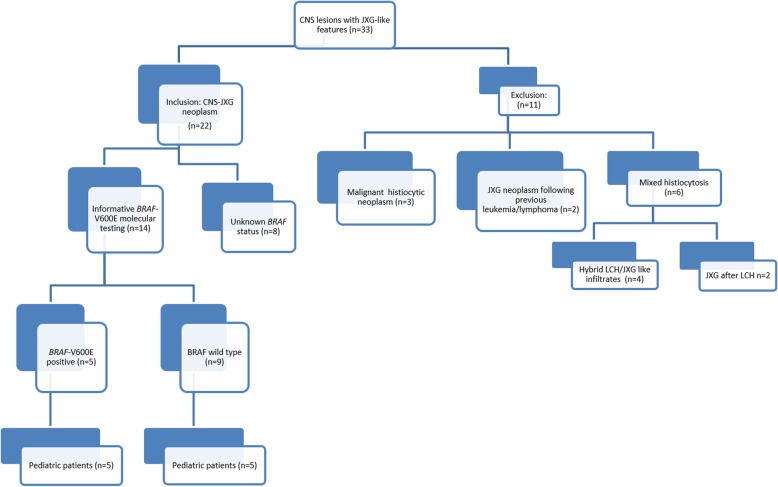
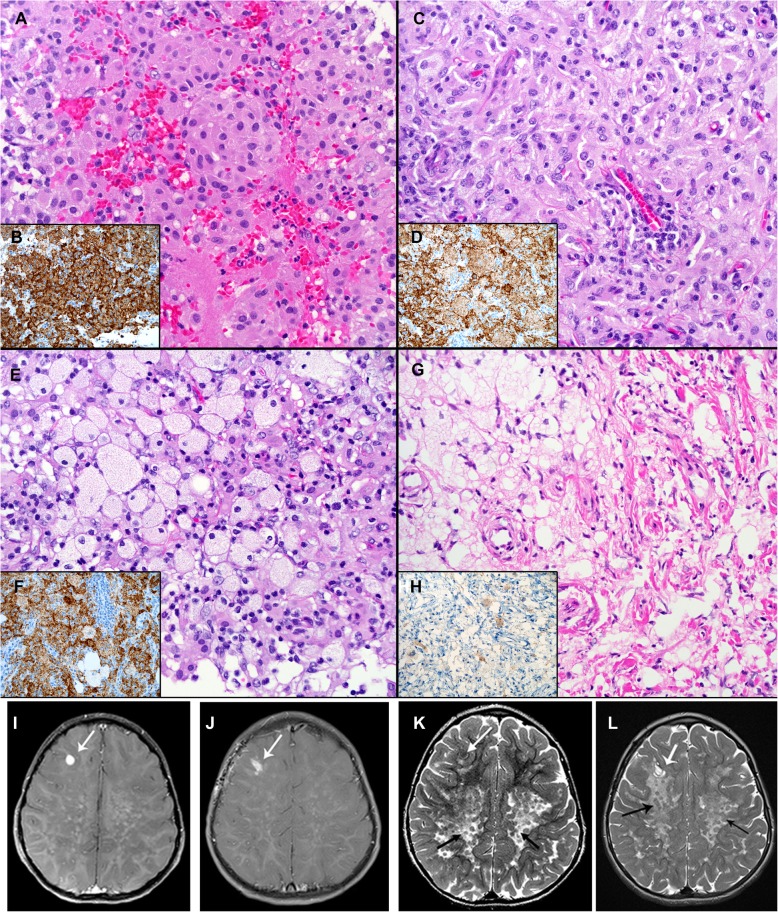
The family of juvenile xanthogranuloma family neoplasms (JXG) with ERK-pathway mutations are now classified within the "L" (Langerhans) group, which includes Langerhans cell histiocytosis (LCH) and Erdheim Chester disease (ECD). Although the BRAF V600E mutation constitutes the majority of molecular alterations in ECD and LCH, only three reported JXG neoplasms, all in male pediatric patients with localized central nervous system (CNS) involvement, are known to harbor the BRAF mutation. This retrospective case series seeks to redefine the clinicopathologic spectrum of pediatric CNS-JXG family neoplasms in the post-BRAF era, with a revised diagnostic algorithm to include pediatric ECD. Twenty-two CNS-JXG family lesions were retrieved from consult files with 64% (n = 14) having informative BRAF V600E mutational testing (molecular and/or VE1 immunohistochemistry). Of these, 71% (n = 10) were pediatric cases (≤18 years) and half (n = 5) harbored the BRAF V600E mutation. As compared to the BRAF wild-type cohort (WT), the BRAF V600E cohort had a similar mean age at diagnosis [BRAF V600E: 7 years (3-12 y), vs. WT: 7.6 years (1-18 y)] but demonstrated a stronger male/female ratio (BRAF V600E: 4 vs WT: 0.67), and had both more multifocal CNS disease ( BRAFV600E: 80% vs WT: 20%) and systemic disease (BRAF V600E: 40% vs WT: none). Radiographic features of CNS-JXG varied but typically included enhancing CNS mass lesion(s) with associated white matter changes in a subset of BRAF V600E neoplasms. After clinical-radiographic correlation, pediatric ECD was diagnosed in the BRAF V600E cohort. Treatment options varied, including surgical resection, chemotherapy, and targeted therapy with BRAF-inhibitor dabrafenib in one mutated case. BRAF V600E CNS-JXG neoplasms appear associated with male gender and aggressive disease presentation including pediatric ECD. We propose a revised diagnostic algorithm for CNS-JXG that includes an initial morphologic diagnosis with a final integrated diagnosis after clinical-radiographic and molecular correlation, in order to identify cases of pediatric ECD. Future studies with long-term follow-up are required to determine if pediatric BRAF V600E positive CNS-JXG neoplasms are a distinct entity in the L-group histiocytosis category or represent an expanded pediatric spectrum of ECD.
幼年黄色肉芽肿家族肿瘤(JXG)的家族成员伴有 ERK 通路突变,现在被归类为“L”(朗格汉斯)组,包括朗格汉斯细胞组织细胞增生症(LCH)和 Erdheim-Chester 病(ECD)。尽管 BRAF V600E 突变构成了 ECD 和 LCH 中大多数分子改变,但已知只有 3 例报告的 JXG 肿瘤,均为男性儿科患者,伴有局限性中枢神经系统(CNS)受累,携带 BRAF 突变。本回顾性病例系列旨在重新定义 BRAF 时代后儿科 CNS-JXG 家族肿瘤的临床病理谱,并提出了包括儿科 ECD 的修订诊断算法。从咨询文件中检索到 22 例 CNS-JXG 家族病变,其中 64%(n=14)具有信息丰富的 BRAF V600E 突变检测(分子和/或 VE1 免疫组化)。其中,71%(n=10)为儿科病例(≤18 岁),一半(n=5)携带 BRAF V600E 突变。与 BRAF 野生型队列(WT)相比,BRAF V600E 队列的诊断年龄中位数相似[BRAF V600E:7 岁(3-12 岁),WT:7.6 岁(1-18 岁)],但男性/女性比例更高(BRAF V600E:4 比 WT:0.67),且更具多发性 CNS 疾病(BRAFV600E:80%比 WT:20%)和全身疾病(BRAF V600E:40%比 WT:无)。CNS-JXG 的影像学特征不同,但在 BRAF V600E 肿瘤的一部分中,通常包括增强的 CNS 肿块病变和相关的白质改变。在临床-影像学相关性后,BRAF V600E 队列中诊断出儿科 ECD。治疗选择多种多样,包括手术切除、化疗和靶向治疗,一例突变病例使用 BRAF 抑制剂 dabrafenib。BRAF V600E CNS-JXG 肿瘤似乎与男性性别和侵袭性疾病表现相关,包括儿科 ECD。我们提出了一种修订后的 CNS-JXG 诊断算法,包括初始形态学诊断,然后在临床-影像学和分子相关性后进行最终综合诊断,以识别儿科 ECD 病例。需要进行长期随访的未来研究,以确定儿科 BRAF V600E 阳性 CNS-JXG 肿瘤是否是 L 组组织细胞增生症类别中的一个独特实体,还是代表 ECD 的扩展儿科谱。