MRI Unit, Division of Radiotherapy and Imaging, The Institute of Cancer Research and the Royal Marsden NHS Foundation Trust, Sutton, UK.
Department of Gynaecological Oncology, The Royal Marsden NHS Foundation Trust, London, UK; St George's University of London, Tooting, London, UK.
Gynecol Oncol. 2020 Jan;156(1):107-114. doi: 10.1016/j.ygyno.2019.10.010. Epub 2019 Nov 2.
Textural features extracted from MRI potentially provide prognostic information additional to volume for influencing surgical management of cervical cancer.
To identify textural features that differ between cervical tumors above and below the volume threshold of eligibility for trachelectomy and determine their value in predicting recurrence in patients with low-volume tumors.
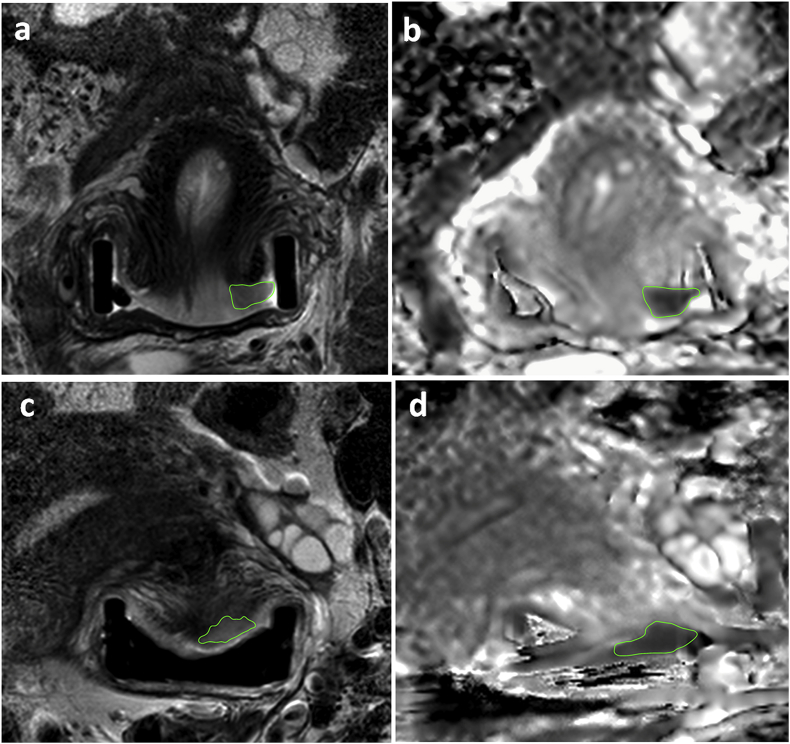
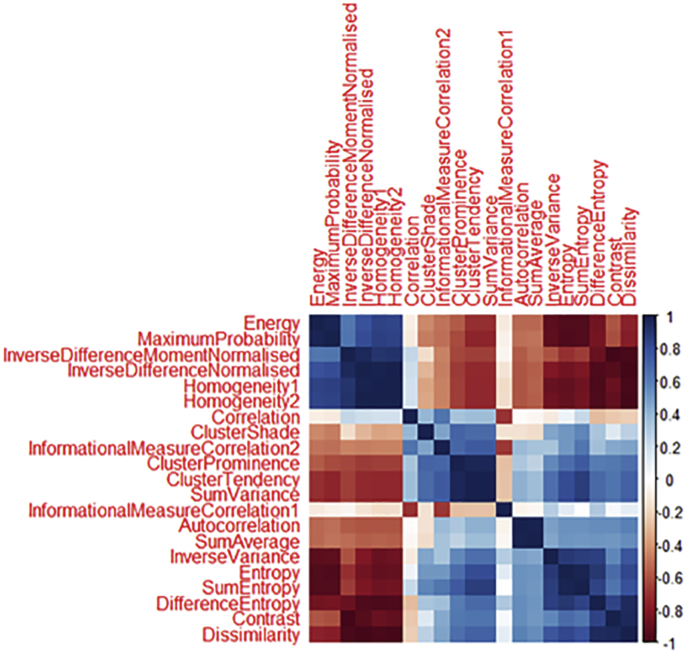
Of 378 patients with Stage1-2 cervical cancer imaged prospectively (3T, endovaginal coil), 125 had well-defined, histologically-confirmed squamous or adenocarcinomas with >100 voxels (>0.07 cm) suitable for radiomic analysis. Regions-of-interest outlined the whole tumor on T2-W images and apparent diffusion coefficient (ADC) maps. Textural features based on grey-level co-occurrence matrices were compared (Mann-Whitney test with Bonferroni correction) between tumors greater (n = 46) or less (n = 79) than 4.19 cm. Clustering eliminated correlated variables. Significantly different features were used to predict recurrence (regression modelling) in surgically-treated patients with low-volume tumors and compared with a model using clinico-pathological features.
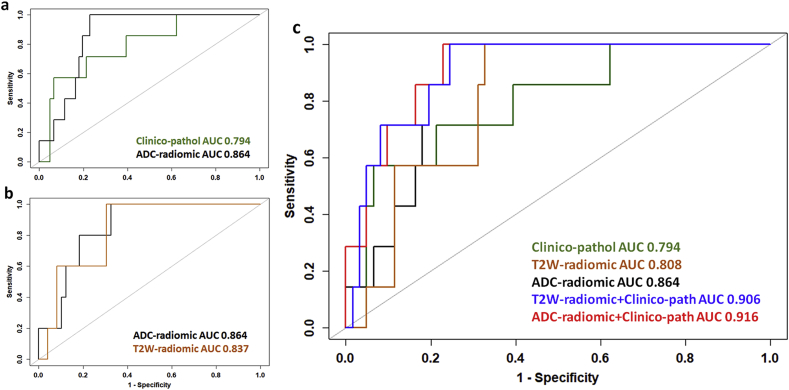
Textural features (Dissimilarity, Energy, ClusterProminence, ClusterShade, InverseVariance, Autocorrelation) in 6 of 10 clusters from T2-W and ADC data differed between high-volume (mean ± SD 15.3 ± 11.7 cm) and low-volume (mean ± SD 1.3 ± 1.2 cm) tumors. (p < 0.02). In low-volume tumors, predicting recurrence was indicated by: Dissimilarity, Energy (ADC-radiomics, AUC = 0.864); Dissimilarity, ClusterProminence, InverseVariance (T2-W-radiomics, AUC = 0.808); Volume, Depth of Invasion, LymphoVascular Space Invasion (clinico-pathological features, AUC = 0.794). Combining ADC-radiomic (but not T2-radiomic) and clinico-pathological features improved prediction of recurrence compared to the clinico-pathological model (AUC = 0.916, p = 0.006). Findings were supported by bootstrap re-sampling (n = 1000).
Textural features from ADC maps and T2-W images differ between high- and low-volume tumors and potentially predict recurrence in low-volume tumors.
从 MRI 提取的纹理特征可能提供比体积更有预后意义的信息,从而影响宫颈癌的手术治疗。
确定肿瘤体积是否超过行宫颈锥切术的阈值,识别肿瘤纹理特征,并确定其在预测低体积肿瘤患者复发中的价值。
对 378 例经前瞻性 MRI 检查的Ⅰ-Ⅱ期宫颈癌患者(3T 场强,经阴道线圈)进行分析,其中 125 例为边界清晰、经组织学证实的鳞癌或腺癌,肿瘤体积>100 个体素(>0.07cm),适用于放射组学分析。在 T2-W 图像和表观扩散系数(ADC)图上勾画感兴趣区(ROI)以勾画整个肿瘤。比较(校正后的 Mann-Whitney 检验)肿瘤体积大于(n=46)或小于(n=79)4.19cm 的肿瘤的纹理特征(灰度共生矩阵)。聚类消除了相关变量。利用在接受手术治疗的低体积肿瘤患者中预测复发的显著不同的特征(回归模型),并与使用临床病理特征的模型进行比较。
在 T2-W 和 ADC 数据的 10 个聚类中,有 6 个聚类的纹理特征(差异性、能量、聚类突出度、聚类阴影、逆方差、自相关)在高体积(平均值±标准差 15.3±11.7cm)和低体积(平均值±标准差 1.3±1.2cm)肿瘤之间存在差异(p<0.02)。在低体积肿瘤中,预测复发的指标包括:差异性、能量(ADC-放射组学,AUC=0.864);差异性、聚类突出度、逆方差(T2-W-放射组学,AUC=0.808);体积、浸润深度、脉管侵犯(临床病理特征,AUC=0.794)。与临床病理模型(AUC=0.916,p=0.006)相比,结合 ADC-放射组学(而非 T2-放射组学)和临床病理特征可提高预测复发的能力。Bootstrap 重采样(n=1000)支持该发现。
高、低体积肿瘤之间的 ADC 图和 T2-W 图像的纹理特征不同,且可能预测低体积肿瘤的复发。