SA MRC Unit on Risk and Resilience in Mental Disorders, Department of Psychiatry, Stellenbosch University, Cape Town, South Africa.
Department of Psychiatry, Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA.
Brain Behav. 2019 Dec;9(12):e01456. doi: 10.1002/brb3.1456. Epub 2019 Nov 6.
A promising approach to reducing the phenotypic heterogeneity of psychiatric disorders involves the identification of homogeneous subtypes. Careful study of comorbidity in obsessive-compulsive disorder (OCD) contributed to the identification of the DSM-5 subtype of OCD with tics. Here we investigated one of the largest available cohorts of clinically diagnosed trichotillomania (TTM) to determine whether subtyping TTM based on comorbidity would help delineate clinically meaningful subgroups.
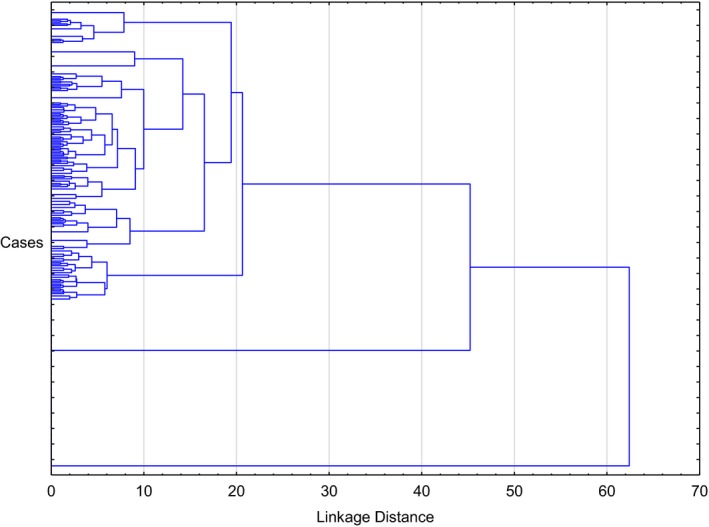
As part of an ongoing international collaboration, lifetime comorbidity data were collated from 304 adults with pathological hair-pulling who fulfilled criteria for DSM-IV-TR or DSM-5 TTM. Cluster analysis (Ward's method) based on comorbidities was undertaken.
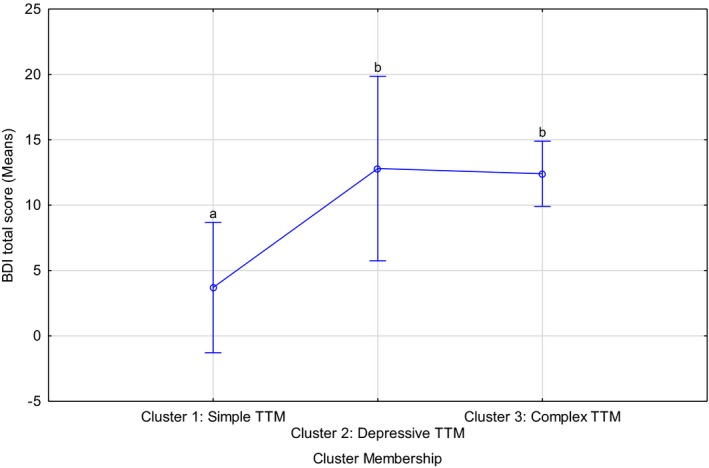
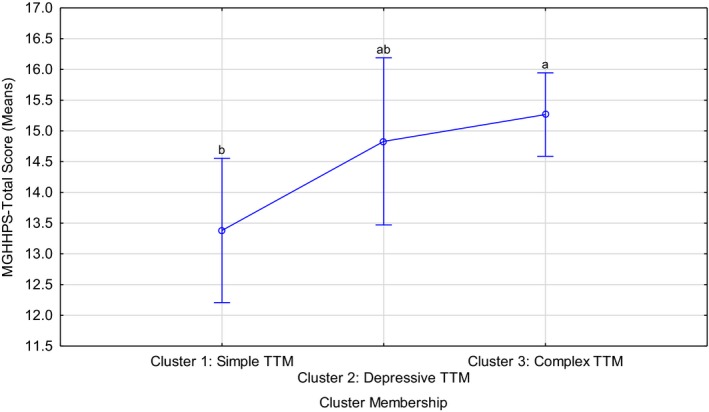
Three clusters were identified, namely Cluster 1: cases without any comorbidities (n = 63, 20.7%) labeled "simple TTM," Cluster 2: cases with comorbid major depressive disorder only (N = 49, 16.12%) labeled "depressive TTM," and Cluster 3: cases presenting with combinations of the investigated comorbidities (N = 192, 63.16%) labeled "complex TTM." The clusters differed in terms of hair-pulling severity (F = 3.75, p = .02; Kruskal-Wallis [KW] p < .01) and depression symptom severity (F = 5.07, p = <.01; KW p < .01), with cases with any comorbidity presenting with increased severity. Analysis of the temporal nature of these conditions in a subset suggested that TTM onset generally preceded major depressive disorder in (subsets of) Clusters 2 and 3.
The findings here are useful in emphasizing that while many TTM patients present without comorbidity, depression is present in a substantial proportion of cases. In clinical practice, it is crucial to assess comorbidity, given the links demonstrated here between comorbidity and symptom severity. Additional research is needed to replicate these findings and to determine whether cluster membership based on comorbidity predicts response to treatment.
减少精神障碍表型异质性的一种有前景的方法涉及到同质亚型的识别。强迫症(OCD)共病的仔细研究促成了 DSM-5 伴抽动障碍 OCD 亚型的识别。在这里,我们研究了最大的一组可用临床诊断拔毛癖(TTM)队列之一,以确定基于共病的 TTM 亚型划分是否有助于划定具有临床意义的亚组。
作为正在进行的国际合作的一部分,从符合 DSM-IV-TR 或 DSM-5 TTM 标准的 304 名病理性拔毛成人中收集了终生共病数据。基于共病的聚类分析(Ward 法)进行了。
确定了三个聚类,即聚类 1:无任何共病的病例(n=63,20.7%),标记为“单纯 TTM”;聚类 2:仅有共患重性抑郁障碍的病例(n=49,16.12%),标记为“抑郁 TTM”;以及聚类 3:表现出所研究共病组合的病例(n=192,63.16%),标记为“复杂 TTM”。聚类在拔毛严重程度方面存在差异(F=3.75,p=0.02;Kruskal-Wallis[KW]p<.01)和抑郁症状严重程度(F=5.07,p<.01;KW p<.01),任何共病的病例都表现出更严重的程度。对这些条件的时间性质的分析表明,在聚类 2 和 3 的(子集)中,TTM 发作通常先于重性抑郁障碍。
这些发现强调了虽然许多 TTM 患者没有共病,但在很大一部分病例中存在抑郁。在临床实践中,鉴于这里显示的共病与症状严重程度之间的联系,评估共病至关重要。需要进一步的研究来复制这些发现,并确定基于共病的聚类成员是否预测对治疗的反应。