Jang Myung Hun, Shin Myung-Jun, Shin Yong Beom
Department of Rehabilitation Medicine, Biomedical Research Institute, Pusan National University Hospital, Busan, Korea.
Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea.
Acute Crit Care. 2019 Feb;34(1):1-13. doi: 10.4266/acc.2019.00444. Epub 2019 Feb 28.
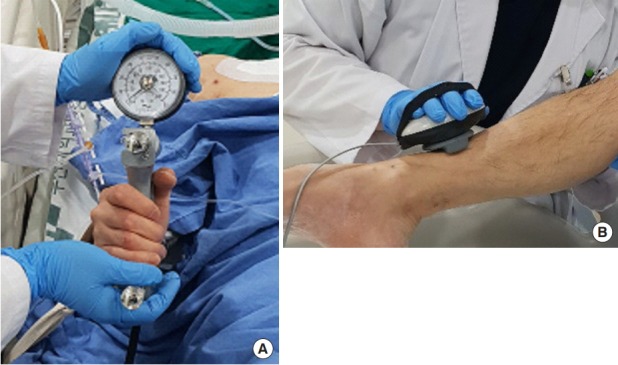
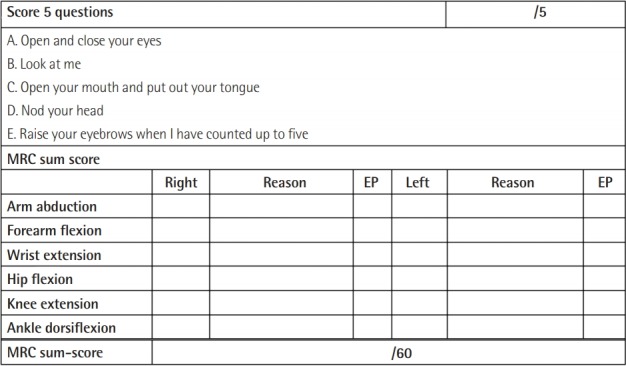
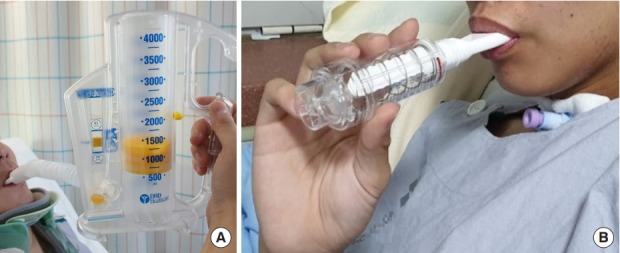
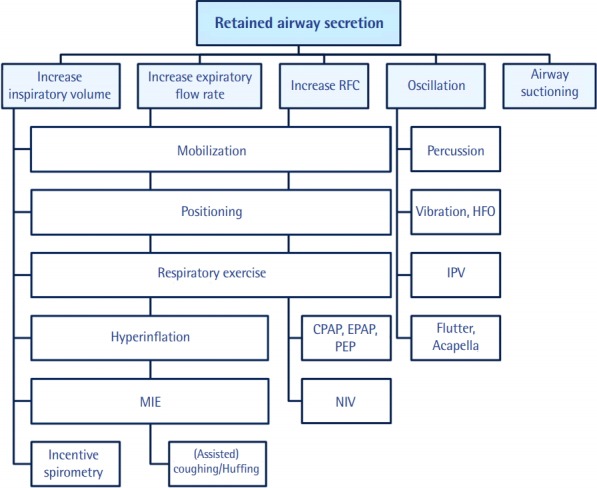
Some patients admitted to the intensive care unit (ICU) because of an acute illness, complicated surgery, or multiple traumas develop muscle weakness affecting the limbs and respiratory muscles during acute care in the ICU. This condition is referred to as ICU-acquired weakness (ICUAW), and can be evoked by critical illness polyneuropathy (CIP), critical illness myopathy (CIM), or critical illness polyneuromyopathy (CIPNM). ICUAW is diagnosed using the Medical Research Council (MRC) sum score based on bedside manual muscle testing in cooperative patients. The MRC sum score is the sum of the strengths of the 12 regions on both sides of the upper and lower limbs. ICUAW is diagnosed when the MRC score is less than 48 points. However, some patients require electrodiagnostic studies, such as a nerve conduction study, electromyography, and direct muscle stimulation, to differentiate between CIP and CIM. Pulmonary rehabilitation in the ICU can be divided into modalities intended to remove retained airway secretions and exercise therapies intended to improve respiratory function. Physical rehabilitation, including early mobilization, positioning, and limb exercises, attenuates the weakness that occurs during critical care. To perform mobilization in mechanically ventilated patients, pretreatment by removing secretions is necessary. It is also important to increase the strength of respiratory muscles and to perform lung recruitment to improve mobilization in patients who are weaned from the ventilator. For these reasons, pulmonary rehabilitation is important in addition to physical therapy. Early recognition of CIP, CIM, and CIPNM and early rehabilitation in the ICU might improve patients' functional recovery and outcomes.
一些因急性疾病、复杂手术或多处创伤而入住重症监护病房(ICU)的患者,在ICU接受急性治疗期间会出现影响四肢和呼吸肌的肌无力。这种情况被称为ICU获得性肌无力(ICUAW),可由重症疾病多发性神经病(CIP)、重症疾病肌病(CIM)或重症疾病多神经肌病(CIPNM)引起。ICUAW通过医学研究委员会(MRC)总分来诊断,该总分基于对合作患者进行床边徒手肌力测试得出。MRC总分是双侧上下肢12个部位肌力的总和。当MRC评分低于48分时可诊断为ICUAW。然而,一些患者需要进行电诊断研究,如神经传导研究、肌电图和直接肌肉刺激,以区分CIP和CIM。ICU中的肺康复可分为旨在清除气道分泌物潴留的方式和旨在改善呼吸功能的运动疗法。物理康复,包括早期活动、体位摆放和肢体锻炼,可减轻重症监护期间出现的肌无力。对于机械通气患者进行活动时,清除分泌物的预处理是必要的。增强呼吸肌力量以及对撤机患者进行肺复张以改善活动能力也很重要。出于这些原因,除了物理治疗外,肺康复也很重要。早期识别CIP、CIM和CIPNM并在ICU早期进行康复可能会改善患者的功能恢复和预后。