Scharrenberg Jan Simon, Yagdiran Ayla, Brinkmann Julia, Brune Maik, Siewe Jan, Jung Norma, Mahabir Esther
Comparative Medicine, Center for Molecular Medicine, University of Cologne, Robert-Koch-Straße 21, 50931, Cologne, Germany.
Department of Orthopedic and Trauma Surgery, University of Cologne, Cologne, Germany.
J Orthop Surg Res. 2019 Nov 14;14(1):367. doi: 10.1186/s13018-019-1420-6.
There is still a challenge in discriminating between vertebral osteomyelitis and degenerative diseases of the spine. To this end, we determined the suitability of soluble urokinase-type plasminogen activator receptor (suPAR) and compared the diagnostic potential of suPAR to CRP.
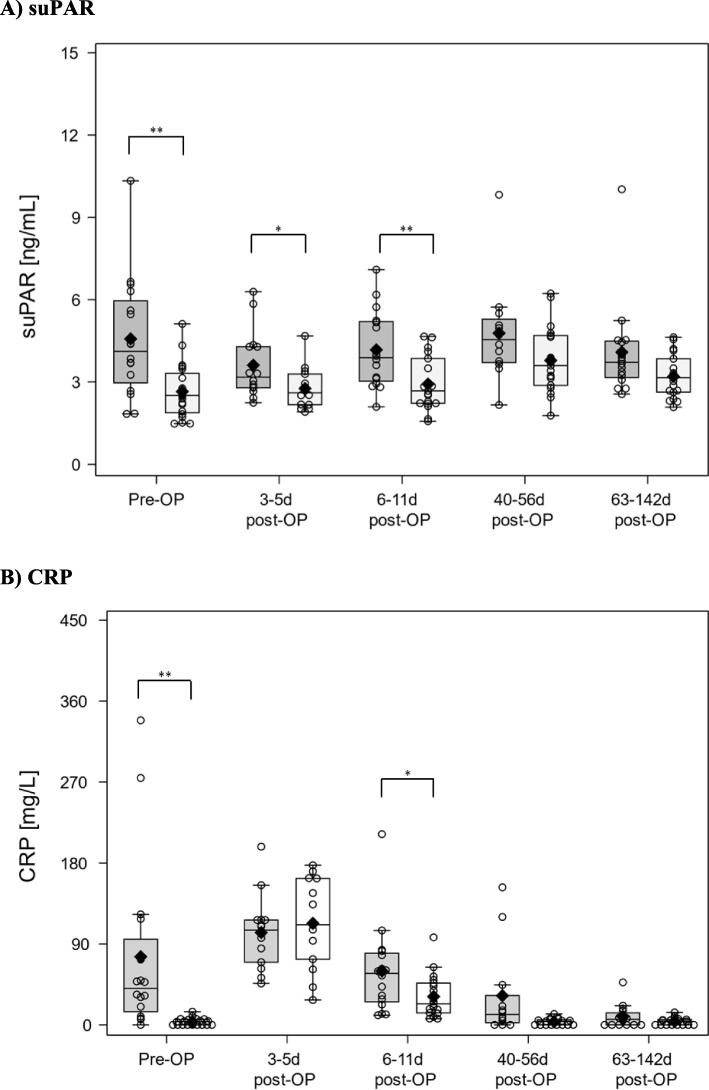
Patients underwent surgical stabilization of the lumbar and/or thoracic spine with removal of one or more affected intervertebral discs, as therapy for vertebral osteomyelitis (n = 16) or for erosive osteochondrosis (control group, n = 20). In this prospective study, we evaluated the suPAR and CRP levels before (pre-OP) and after surgery (post-OP) on days 3-5, 6-11, 40-56, and 63-142.
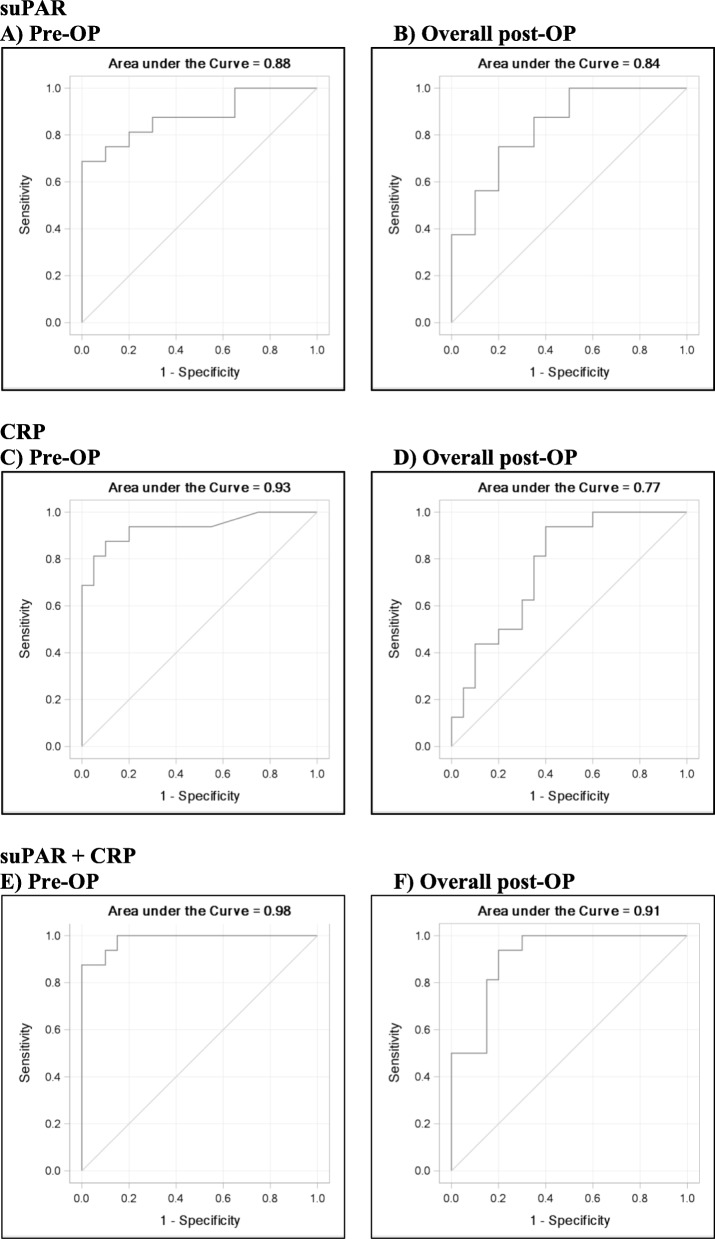
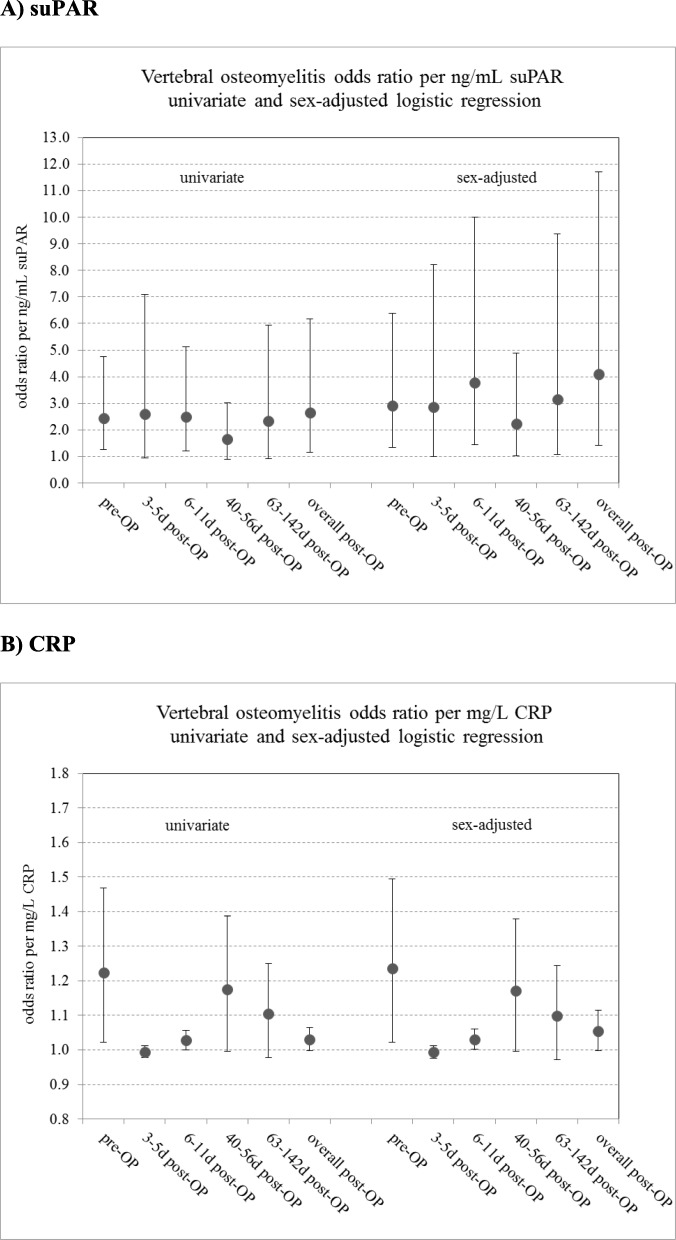
The suPAR levels in vertebral osteomyelitis patients were significantly higher than those from controls pre-OP, 3-5 days post-OP, and 6-11 days post-OP. Significantly higher CRP levels were observed in the vertebral osteomyelitis group than in the controls pre-OP and 6-11 days post-OP. Levels of suPAR and CRP correlated positively in all patients in the pre-OP period: r = 0.63 (95% CI: 0.37-0.79), p < 0.0001. The values for the area under the receiver operating characteristics curve (AUC) for pre-OP and the overall model post-OP were 0.88 (95% CI: 0.76-1.00) and 0.84 (95% CI: 0.71-0.97) for suPAR, 0.93 (95% CI: 0.85-1.00) and 0.77 (95% CI: 0.62-0.93) for CRP, and 0.98 (95% CI: 0.96-1.00) and 0.91 (95% CI: 0.82-1.00) for the combination of suPAR and CRP. The AUC for suPAR pre-OP revealed an optimum cut-off value, sensitivity, specificity, NPV, and PPV of 2.96 ng/mL, 0.69, 1.00, 0.80, and 1.00, respectively. For CRP, these values were 11.58 mg/L, 0.88, 0.90, 0.90, and 0.88, respectively.
The present results show that CRP is more sensitive than suPAR whereas suPAR is more specific than CRP. Moreso, our study demonstrated that improvement in the diagnostic power for discrimination of vertebral osteomyelitis and degenerative diseases of the spine can be achieved by a combination of both suPAR and CRP.
ClinicalTrials.gov, NCT02554227, posted Sept. 18, 2015, and updated Aug. 13, 2019.
鉴别脊椎骨髓炎和脊柱退行性疾病仍然是一项挑战。为此,我们确定了可溶性尿激酶型纤溶酶原激活物受体(suPAR)的适用性,并比较了suPAR与CRP的诊断潜力。
患者接受腰椎和/或胸椎手术固定,并切除一个或多个受影响的椎间盘,作为脊椎骨髓炎(n = 16)或侵蚀性骨软骨病(对照组,n = 20)的治疗方法。在这项前瞻性研究中,我们评估了术前(术前)以及术后第3 - 5天、6 - 11天、40 - 56天和63 - 142天的suPAR和CRP水平。
脊椎骨髓炎患者的suPAR水平在术前、术后3 - 5天和术后6 - 11天显著高于对照组。脊椎骨髓炎组术前和术后6 - 11天的CRP水平显著高于对照组。术前所有患者的suPAR和CRP水平呈正相关:r = 0.63(95%CI:0.37 - 0.79),p < 0.0001。术前suPAR的受试者操作特征曲线(AUC)下面积值和术后总体模型分别为0.88(95%CI:0.76 - 1.00)和0.84(95%CI:0.71 - 0.97),CRP分别为0.93(95%CI:0.85 - 1.00)和0.77(95%CI:0.62 - 0.93),suPAR和CRP联合检测分别为0.98(95%CI:(95%CI:0.96 - 1.00)和0.91(95%CI:0.82 - 1.00)。术前suPAR的AUC显示最佳截断值、敏感性、特异性、阴性预测值和阳性预测值分别为2.96 ng/mL、0.69、1.00、0.80和1.00。对于CRP,这些值分别为11.58 mg/L、0.88、0.90、0.90和0.88。
目前的结果表明,CRP比suPAR更敏感,而suPAR比CRP更具特异性。此外,我们的研究表明,联合使用suPAR和CRP可以提高鉴别脊椎骨髓炎和脊柱退行性疾病的诊断能力。
ClinicalTrials.gov,NCT02554227,于(2015年9月18日发布,并于2019年8月13日更新。