Pires Hudson Henrique Gomes, Neves Fábio Fernandes, Pazin-Filho Antonio
Department of Internal Medicine, Urgency and Emergency Discipline, Triangulo Mineiro Medical School, Federal University of Triangulo Mineiro, Avenida Getúlio Guaritá, 159, Bairro, Nossa Senhora da Abadia, Uberaba, Minas Gerais, 38025-440, Brazil.
Department of Internal Medicine, São Carlos Medical School, Federal University of São Carlos, São Carlos, Brazil.
Int J Emerg Med. 2019 Nov 21;12(1):36. doi: 10.1186/s12245-019-0252-9.
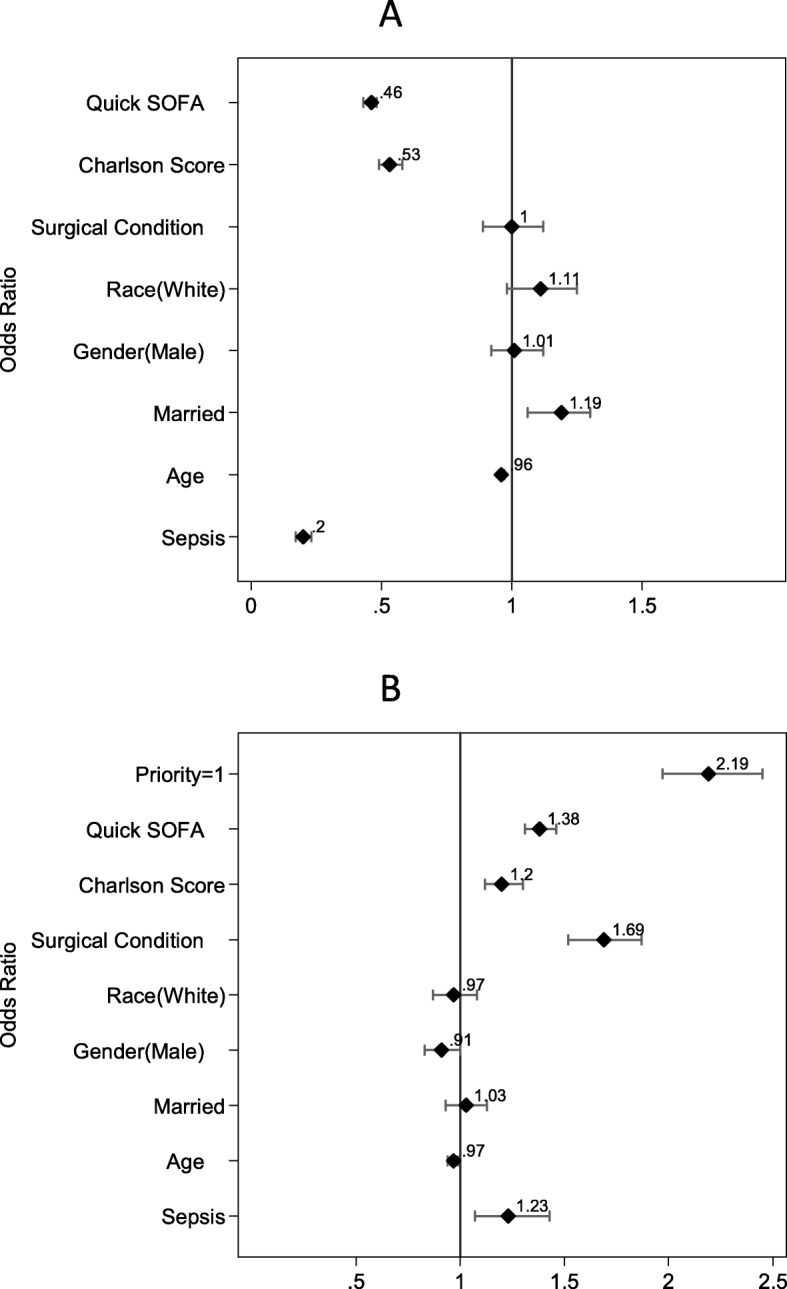
Sepsis is a major public health problem, with a growing incidence and mortality rates still close to 30% in severe cases. The speed and adequacy of the treatment administered in the first hours of sepsis, particularly access to intensive care, are important to reduce mortality. This study compared the triage strategies and intensive care rationing between septic patients and patients with other indications of intensive care. This study included all patients with signs for intensive care, enrolled in the intensive care management system of a Brazilian tertiary public emergency hospital, from January 1, 2010, to December 31, 2016. The intensivist periodically evaluated the requests, prioritizing them according to a semi-quantitative scale. Demographic data, Charlson Comorbidity Index (CCI), Sequential Organ Failure Assessment (SOFA), and quick SOFA (qSOFA), as well as surgical interventions, were used as possible confounding factors in the construction of incremental logistic regression models for prioritization and admission to intensive care outcomes.
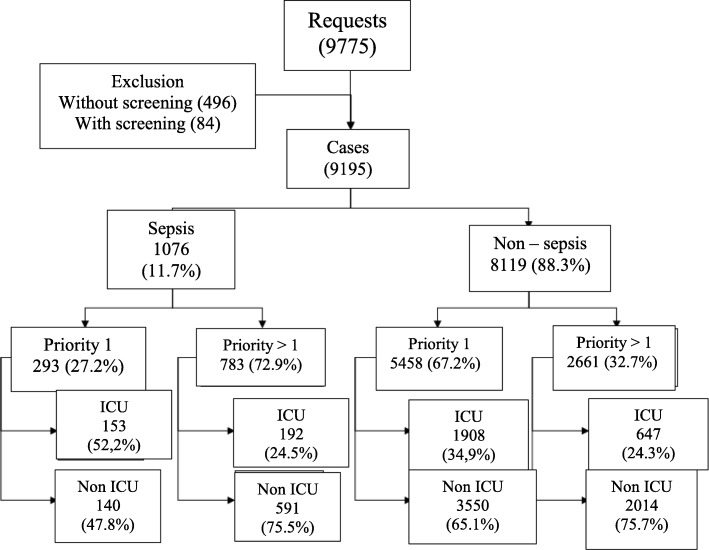
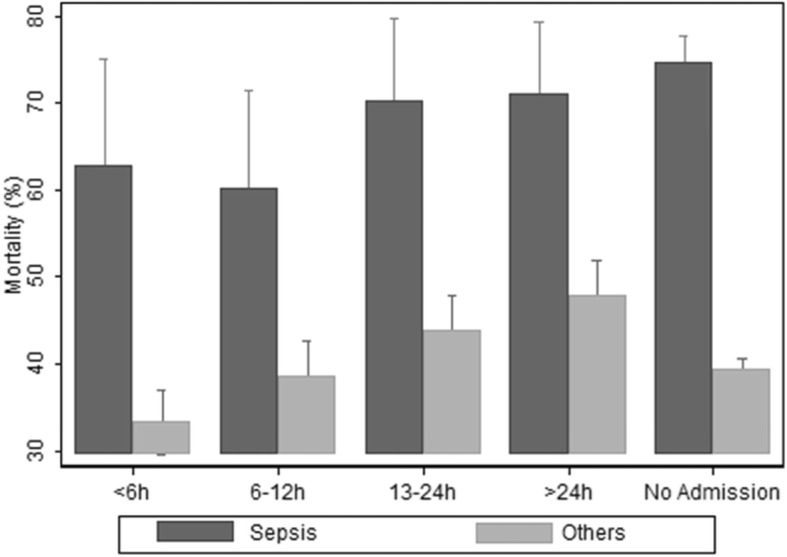
The study analyzed 9195 ICU requests; septic patients accounted for 1076 cases (11.7%), 293 (27.2%) of which were regarded as priority 1. Priority 1 septic patients were more frequently hospitalized in the ICU than nonseptic patients (52.2% vs. 34.9%, p < 0.01). Septic patients waited longer for the vacancy, with a median delay time of 43.9 h (interquartile range 18.2-108.0), whereas nonseptic patients waited 32.5 h (interquartile range 11.5-75.8)-p < 0.01. Overall mortality was significantly higher in the septic group than in the group of patients with other indications for intensive care (72.3% vs. 39.8%, p < 0.01). This trend became more evident after the multivariate analysis, and the mortality odds ratio was almost three times higher in septic patients (2.7, 2.3-3.1).
Septic patients had a lower priority for ICU admission and longer waiting times for an ICU vacancy than patients with other critical conditions. Overall, this implied a 2.7-fold increased risk of mortality in septic patients.
脓毒症是一个重大的公共卫生问题,其发病率不断上升,严重病例的死亡率仍接近30%。在脓毒症发病后的最初几个小时内给予治疗的速度和充分性,尤其是进入重症监护病房的机会,对于降低死亡率至关重要。本研究比较了脓毒症患者与其他需要重症监护的患者之间的分诊策略和重症监护资源分配情况。本研究纳入了2010年1月1日至2016年12月31日期间在巴西一家三级公立急诊医院的重症监护管理系统中登记的所有有重症监护指征的患者。重症监护医生定期评估这些请求,并根据半定量量表对其进行优先级排序。人口统计学数据、查尔森合并症指数(CCI)、序贯器官衰竭评估(SOFA)和快速SOFA(qSOFA)以及手术干预措施,被用作构建用于确定重症监护优先级和入住重症监护病房结果的增量逻辑回归模型时可能的混杂因素。
该研究分析了9195份重症监护病房请求;脓毒症患者占1076例(11.7%),其中293例(27.2%)被视为一级优先。一级优先的脓毒症患者比非脓毒症患者更频繁地入住重症监护病房(52.2%对34.9%,p<0.01)。脓毒症患者等待空位的时间更长,中位延迟时间为43.9小时(四分位间距18.2 - 108.0),而非脓毒症患者等待32.5小时(四分位间距11.5 - 75.8),p<0.01。脓毒症组的总体死亡率显著高于其他需要重症监护的患者组(72.3%对39.8%,p<0.01)。在多变量分析后,这种趋势变得更加明显,脓毒症患者的死亡比值比几乎高出三倍(2.7,2.3 - 3.1)。
与其他危急情况的患者相比,脓毒症患者入住重症监护病房的优先级较低,等待重症监护病房空位的时间更长。总体而言,这意味着脓毒症患者的死亡风险增加了2.7倍。