Sunnybrook Research Institute, Sunnybrook Health Sciences Centre, University of Toronto, 2075 Bayview Ave., Room M1, Toronto, 102, Canada.
University of Western Australia, School of Surgery, Perth, Australia.
J Otolaryngol Head Neck Surg. 2019 Nov 21;48(1):65. doi: 10.1186/s40463-019-0388-x.
Knowledge of the cochlear implant array's precise position is important because of the correlation between electrode position and speech understanding. Several groups have provided recent image processing evidence to determine scalar translocation, angular insertion depth, and cochlear duct length (CDL); all of which are being used for patient-specific programming. Cone beam computed tomography (CBCT) is increasingly used in otology due to its superior resolution and low radiation dose. Our objectives are as followed: 1.Validate CBCT by measuring cochlear metrics, including basal turn diameter (A-value) and lateral wall cochlear duct length at different angular intervals and comparing it against microcomputed CT (uCT).2.Explore the relationship between measured lateral wall cochlear duct length at different angular intervals and insertion depth among 3 different length electrodes using CBCT.
The study was performed using fixed human cadaveric temporal bones in a tertiary academic centre. Ten temporal bones were subjected to the standard facial recess approach for cochlear implantation and imaged by CBCT followed by uCT. Measurements were performed on a three-dimensional reconstructed model of the cochlea. Sequential insertion of 3 electrodes (Med-El Flex24, 28 and Soft) was then performed in 5 bones and reimaged by CBCT. Statistical analysis was performed using Pearson's correlation.
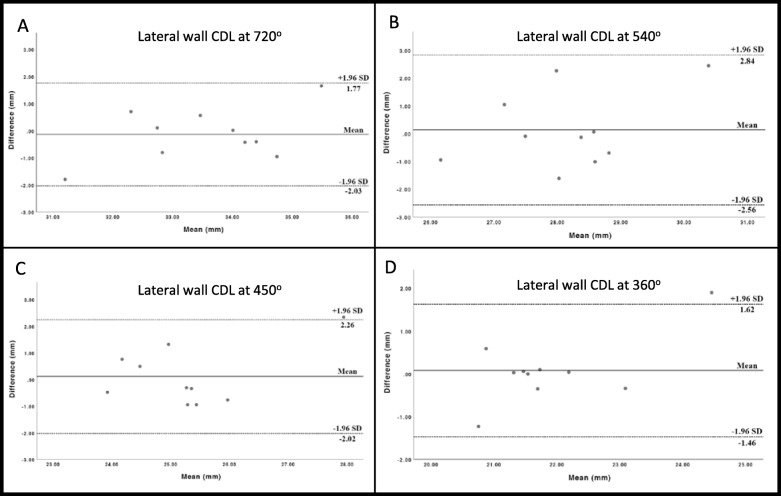
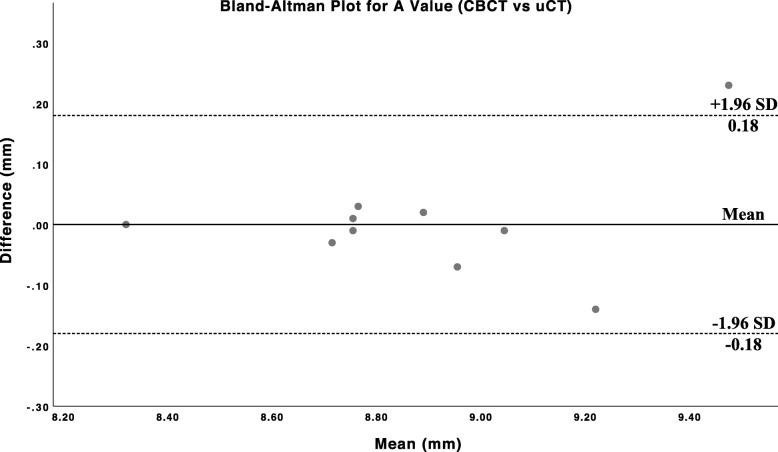
There was good agreement between CBCT and uCT for cochlear metrics, validating the precision of CBCT against the current gold standard uCT in imaging. The A-value recorded by both modalities showed a high degree of linear correlation and did not differ by more than 0.23 mm in absolute values. For the measurement of lateral wall CDL at various points along the cochlea, there was a good correlation between both modalities at 360 deg and 720 deg (r = 0.85, p < 0.01 and r = 0.79, p < 0.01). The Flex24 electrode displayed consistent insertion depth across different bones.
CBCT reliably performs cochlear metrics and measures electrode insertion depth. The low radiation dose, fast acquisition time, diminished metallic artifacts and portability of CBCT make it a valid option for imaging in cochlear implant surgery.
由于电极位置与言语理解之间存在相关性,了解 Cochlear 植入物阵列的精确位置很重要。 有几个研究小组最近提供了图像处理证据,以确定标量移位、角插入深度和耳蜗管长度(CDL); 所有这些都用于患者特定的编程。 由于其优越的分辨率和低辐射剂量,锥形束计算机断层扫描(CBCT)在耳科学中越来越多地使用。 我们的目标如下:1. 通过测量耳蜗参数来验证 CBCT,包括在不同角度间隔处的基底转直径(A 值)和外侧壁耳蜗管长度,并将其与微计算机断层扫描(uCT)进行比较。2. 探索使用 CBCT 测量不同角度间隔处的外侧壁耳蜗管长度与 3 个不同长度电极的插入深度之间的关系。
该研究在一家三级学术中心的固定人体尸体颞骨上进行。 10 个颞骨接受 Cochlear 植入的标准面神经隐窝入路,并通过 CBCT 成像,然后进行 uCT 成像。 在耳蜗的三维重建模型上进行测量。 然后在 5 个骨头中连续插入 3 个电极(Med-El Flex24、28 和 Soft),并通过 CBCT 重新成像。 使用 Pearson 相关进行统计分析。
CBCT 和 uCT 对耳蜗参数的测量结果吻合良好,验证了 CBCT 在成像方面对当前金标准 uCT 的精确性。 两种模态记录的 A 值显示出高度的线性相关性,绝对值相差不超过 0.23 毫米。 对于耳蜗各部位外侧壁 CDL 的测量,两种模态在 360°和 720°之间相关性良好(r=0.85,p<0.01 和 r=0.79,p<0.01)。 Flex24 电极在不同骨头中具有一致的插入深度。
CBCT 可靠地执行耳蜗参数测量和电极插入深度测量。 低辐射剂量、快速采集时间、减少的金属伪影和 CBCT 的便携性使其成为 Cochlear 植入手术成像的有效选择。