Hu Jie, Spina Stefano, Zadek Francesco, Kamenshchikov Nikolay O, Bittner Edward A, Pedemonte Juan, Berra Lorenzo
Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, 55 Fruit Street, Boston, MA, USA.
Department of Critical Care Medicine, Chinese PLA General Hospital, 28 Fuxing Road, Beijing, China.
Ann Intensive Care. 2019 Nov 21;9(1):129. doi: 10.1186/s13613-019-0605-9.
The effect of nitric oxide (NO) on renal function is controversial in critical illness. We performed a systematic meta-analysis and trial sequential analysis to determine the effect of NO gas on renal function and other clinical outcomes in patients requiring cardiopulmonary bypass (CPB). The primary outcome was the relative risk (RR) of acute kidney injury (AKI), irrespective of the AKI stage. The secondary outcome was the mean difference (MD) in the length of ICU and hospital stay, the RR of postoperative hemorrhage, and the MD in levels of methemoglobin. Trial sequential analysis (TSA) was performed for the primary outcome.
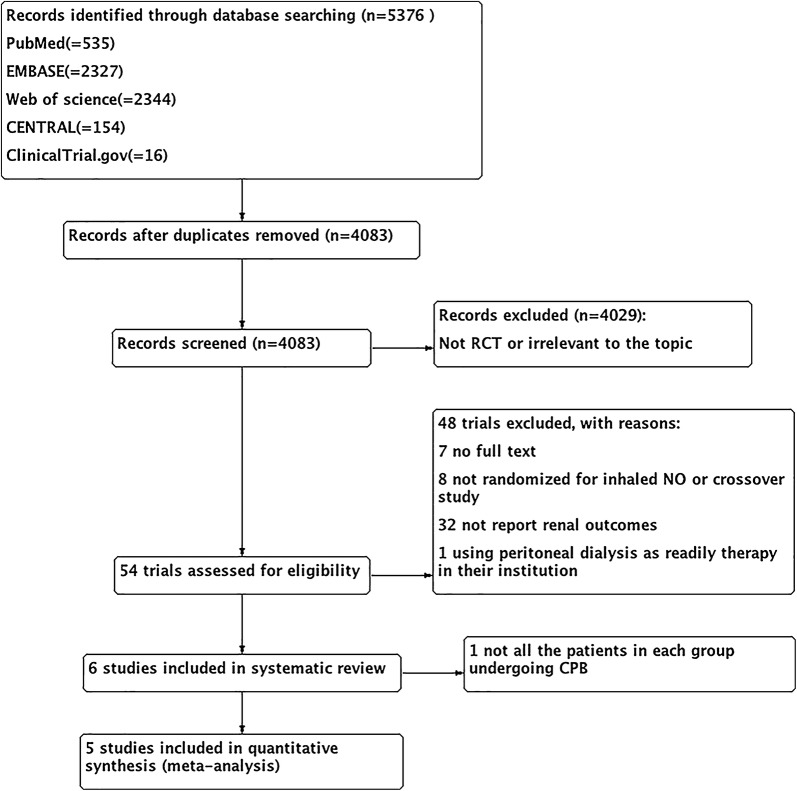
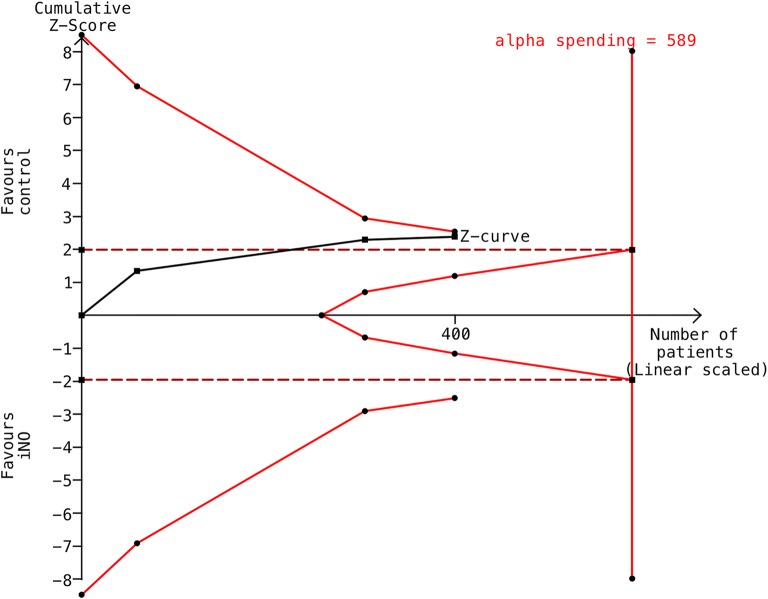
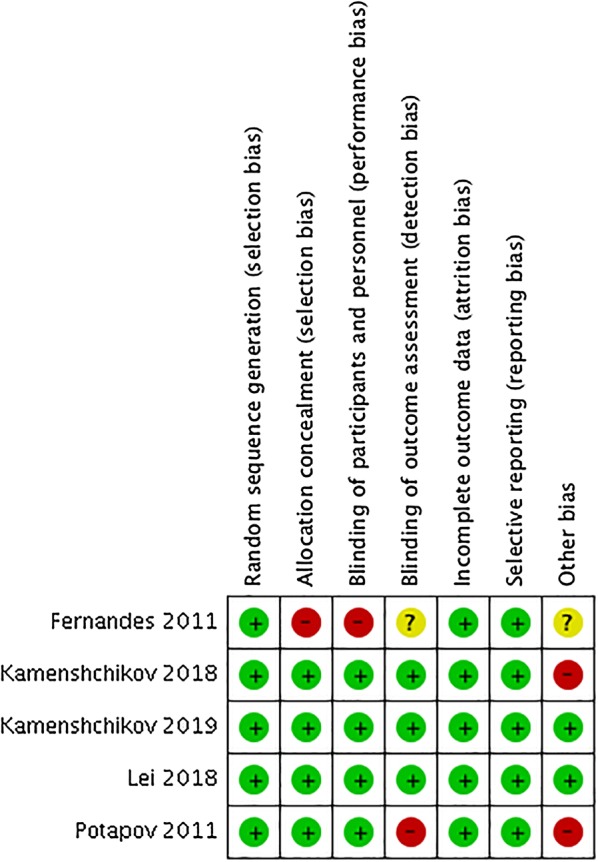
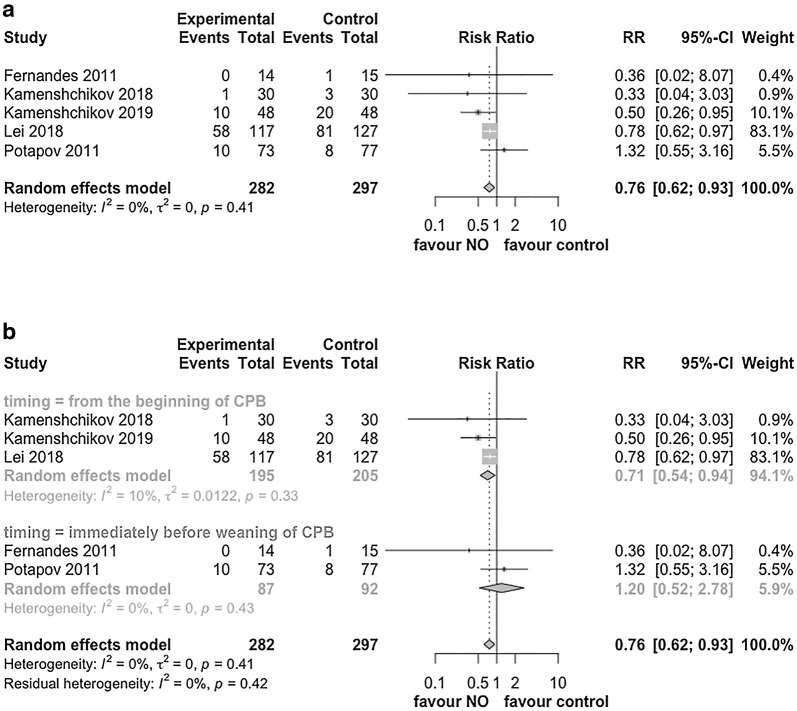
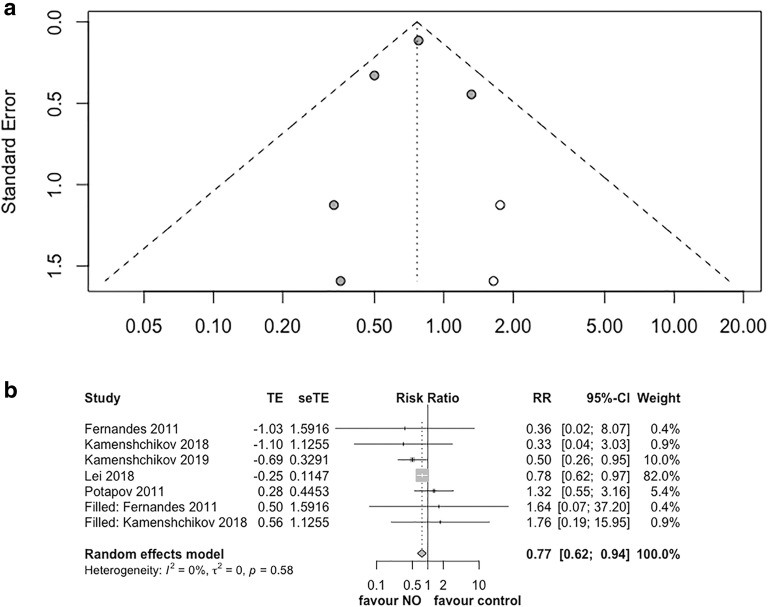
54 trials were assessed for eligibility and 5 studies (579 patients) were eligible for meta-analysis. NO was associated with reduced risk of AKI (RR 0.76, 95% confidential interval [CI], 0.62 to 0.93, I = 0%). In the subgroup analysis by NO initiation timing, NO did not decrease the risk of AKI when started at the end of CPB (RR 1.20, 95% CI 0.52-2.78, I = 0%). However, NO did significantly reduce the risk of AKI when started from the beginning of CPB (RR 0.71, 95% CI 0.54-0.94, I = 10%). We conducted TSA based on three trials (400 patients) using KDIGO criteria and with low risk of bias. TSA indicated a CI of 0.50-1.02 and an optimal information size of 589 patients, suggesting a lack of definitive conclusion. Furthermore, NO does not affect the length of ICU and hospital stay or the risk of postoperative hemorrhage. NO slightly increased the level of methemoglobin at the end of CPB (MD 0.52%, 95% CI 0.27-0.78%, I = 90%), but it was clinically negligible.
NO appeared to reduce the risk of postoperative AKI in patients undergoing CPB. Additional studies are required to ascertain the finding and further determine the dosage, timing and duration of NO administration.
在危重症中,一氧化氮(NO)对肾功能的影响存在争议。我们进行了一项系统的荟萃分析和试验序贯分析,以确定NO气体对需要体外循环(CPB)的患者的肾功能及其他临床结局的影响。主要结局是急性肾损伤(AKI)的相对风险(RR),不考虑AKI分期。次要结局是重症监护病房(ICU)和住院时间的平均差(MD)、术后出血的RR以及高铁血红蛋白水平的MD。对主要结局进行了试验序贯分析(TSA)。
评估了54项试验的 eligibility,5项研究(579例患者)符合荟萃分析条件。NO与降低AKI风险相关(RR 0.76,95%置信区间[CI],0.62至0.93,I = 0%)。在按NO起始时间进行的亚组分析中,CPB结束时开始使用NO并未降低AKI风险(RR 1.20,95% CI 0.52 - 2.78,I = 0%)。然而,CPB开始时就开始使用NO确实显著降低了AKI风险(RR 0.71,95% CI 0.54 - 0.94,I = 10%)。我们基于三项试验(400例患者)采用KDIGO标准且偏倚风险较低进行了TSA。TSA显示CI为0.50 - 1.02,最佳信息规模为589例患者,表明缺乏明确结论。此外,NO不影响ICU和住院时间或术后出血风险。CPB结束时NO使高铁血红蛋白水平略有升高(MD 0.52%,95% CI 0.27 - 0.78%,I = 90%),但临床上可忽略不计。
NO似乎可降低接受CPB患者术后AKI的风险。需要进一步研究以证实这一发现,并进一步确定NO给药的剂量、时间和持续时间。