Department of Surgery and Center for Minimally Invasive Surgery, Academic Teaching Hospital of Charité Medical School, Vivantes Hospital, Neue Bergstrasse 6, 13585, Berlin, Germany.
Department of Surgery, Manchester University NHS Foundation Trust, Manchester, M13 9WL, UK.
Hernia. 2019 Dec;23(6):1081-1091. doi: 10.1007/s10029-019-02062-z. Epub 2019 Nov 21.
The Accreditation and Certification of Hernia Centers and Surgeons (ACCESS) Group of the European Hernia Society (EHS) recognizes that there is a growing need to train specialist abdominal wall surgeons. The most important and relevant argument for this proposal and statement is the growing acceptance of the increasing complexity of abdominal wall surgery due to newer techniques, more challenging cases and the required 'tailored' approach to such surgery. There is now also an increasing public awareness with social media, whereby optimal treatment results are demanded by patients. However, to date the complexity of abdominal wall surgery has not been properly or adequately defined in the current literature.
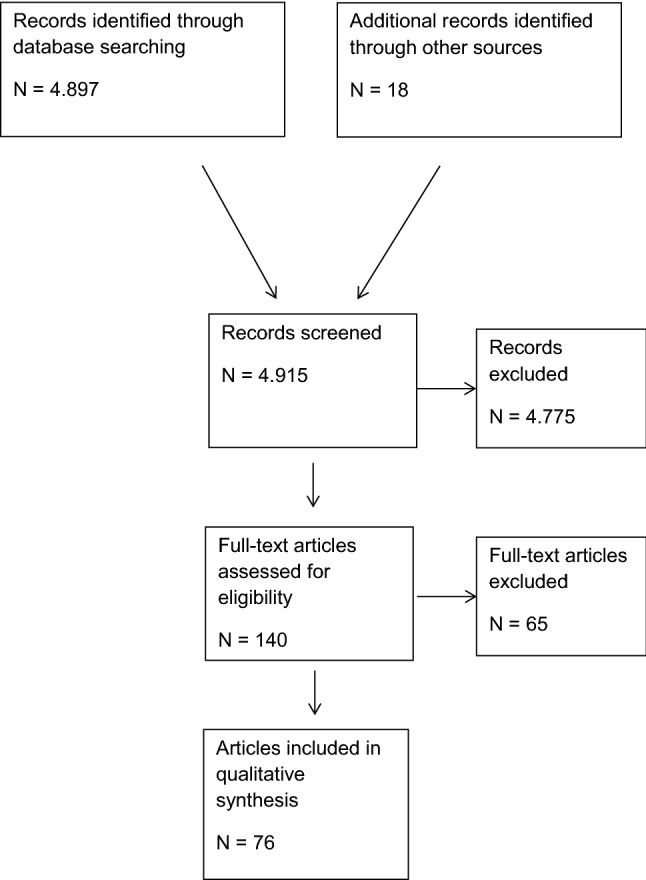
A systematic search of the available literature was performed in May 2019 using Medline, PubMed, Scopus, Embase, Springer Link, and the Cochrane Library, with 75 publications identified as relevant. In addition, an analysis of data from the Herniamed Hernia Registry was performed. The percentage of patients with hernia- or patient-related characteristics which unfavorably impacted the outcome of inguinal and incisional hernia repair was also calculated.
All present guidelines for abdominal wall surgery recommend the utilization of a 'tailored' approach. This relies on the prerequisite that any surgical technique used has already been mastered, as well as the recognized learning curves for each of the several techniques that can be used for both inguinal hernia (Lichtenstein, TEP, TAPP, Shouldice) and incisional hernia repairs (laparoscopic IPOM, open sublay, open IPOM, open onlay, open or endoscopic component separation technique). Other hernia- and patient-related characteristics that have recognized complexity include emergency surgery, obesity, recurrent hernias, bilateral inguinal hernias, groin hernia in women, scrotal hernias, large defects, high ASA scores, > 80 years of age, increased medical risk factors and previous lower abdominal surgery. The proportion of patients with at least one of these characteristics in the Herniamed Hernia Registry in the case of both inguinal and incisional hernia is noted to be relatively high at around 70%. In general surgery training approximately 50-100 hernia repairs on average are performed by each trainee, with around only 25 laparo-endoscopic procedures.
A tailored approach is now employed and seen more so in hernia surgery and this fact is referred to and highlighted in the contemporaneous hernia guidelines published to date. In addition, with the increasing complexity of abdominal wall surgery, the number of procedures actually performed by trainees is no longer considered adequate to overcome any recognized learning curve. Therefore, to supplement general surgery training young surgeons should be offered a clinical fellowship to obtain an additional qualification as an abdominal wall surgeon and thus improve their clinical and operative experience under supervision in this field. Practicing general surgeons with a special interest in hernia surgery can undertake intensive further training in this area by participating in clinical work shadowing in hernia centers, workshops and congresses.
疝和腹壁外科学会(EHS)的疝中心和外科医生认证和认证(ACCESS)小组认识到,培训专业腹壁外科医生的需求日益增长。提出这一建议和声明的最重要和最相关的论点是,由于新技术、更具挑战性的病例以及对这种手术的“量身定制”方法的要求,腹壁手术的复杂性日益增加。现在,社交媒体也提高了公众的认识,患者要求获得最佳的治疗效果。然而,迄今为止,当前文献中并未对腹壁手术的复杂性进行适当或充分的定义。
2019 年 5 月,使用 Medline、PubMed、Scopus、Embase、Springer Link 和 Cochrane 图书馆对现有文献进行了系统搜索,确定了 75 篇相关文献。此外,还对 Herniamed 疝登记处的数据进行了分析。还计算了与疝或患者相关的特征的百分比,这些特征对腹股沟疝和切口疝修复的结果产生了不利影响。
所有现有的腹壁手术指南都建议采用“量身定制”的方法。这依赖于以下前提,即使用的任何手术技术都已掌握,以及每种可用于腹股沟疝(Lichtenstein、TEP、TAPP、Shouldice)和切口疝修复(腹腔镜 IPOM、开放式下衬垫、开放式 IPOM、开放式上衬垫、开放式或内镜组件分离技术)的技术的公认学习曲线。其他与疝和患者相关的具有公认复杂性的特征包括急诊手术、肥胖、复发性疝、双侧腹股沟疝、女性腹股沟疝、阴囊疝、大缺损、ASA 评分高、>80 岁、增加的医疗风险因素和先前的下腹部手术。在 Herniamed 疝登记处,腹股沟疝和切口疝的患者中至少有一个这些特征的比例相对较高,约为 70%。在普通外科培训中,每位受训者平均进行 50-100 例疝修复,腹腔镜内镜手术约为 25 例。
现在采用了量身定制的方法,在疝外科中更为常见,这一事实在迄今为止发表的当代疝指南中有所提及和强调。此外,随着腹壁外科手术复杂性的增加,受训者实际进行的手术数量不再被认为足以克服任何公认的学习曲线。因此,为了补充普通外科培训,应向年轻外科医生提供临床研究员职位,以获得腹壁外科医生的额外资格,从而在该领域的监督下提高他们的临床和手术经验。对疝外科有特殊兴趣的普通外科医生可以通过参加疝中心的临床工作观摩、研讨会和大会来接受该领域的强化进一步培训。