Institute for Clinical Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Department of Neurology, Hospital São Sebastião, Centro Hospitalar de Entre o Douro e Vouga, Santa Maria da Feira, Portugal.
Epilepsia. 2019 Dec;60(12):2437-2447. doi: 10.1111/epi.16381. Epub 2019 Nov 21.
A large-scale, double-blind trial (SP0993; NCT01243177) demonstrated that lacosamide was noninferior to controlled-release carbamazepine (carbamazepine-CR) in terms of efficacy, and well tolerated as first-line monotherapy in patients (≥16 years of age) with newly diagnosed epilepsy. We report primary safety outcomes from the double-blind extension of the noninferiority trial (SP0994; NCT01465997) and post hoc analyses of pooled long-term safety and efficacy data from both trials.
Patients were randomized 1:1 to lacosamide or carbamazepine-CR. Doses were escalated (lacosamide: 200/400/600 mg/d; carbamazepine-CR: 400/800/1200 mg/d) based on seizure control. Eligible patients continued randomized treatment in the extension. Primary outcomes of the extension were treatment-emergent adverse events (TEAEs), serious TEAEs, and discontinuations due to TEAEs. Post hoc analyses of data from combined trials included 12- and 24-month seizure freedom and TEAEs by number of comorbid conditions.
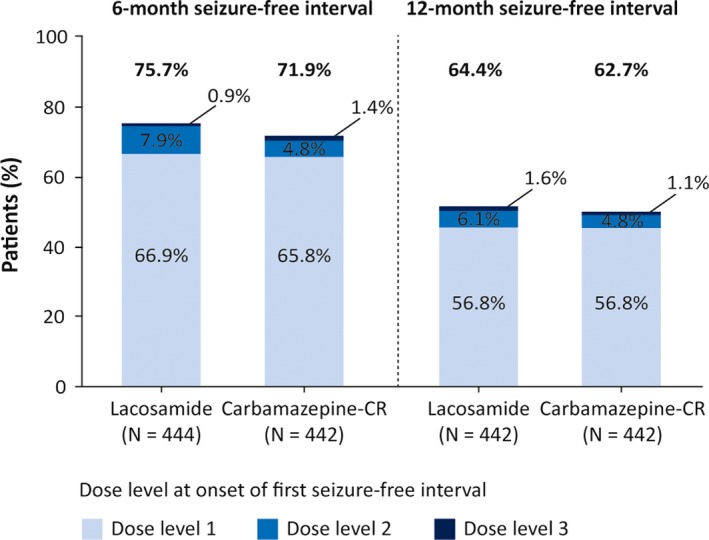
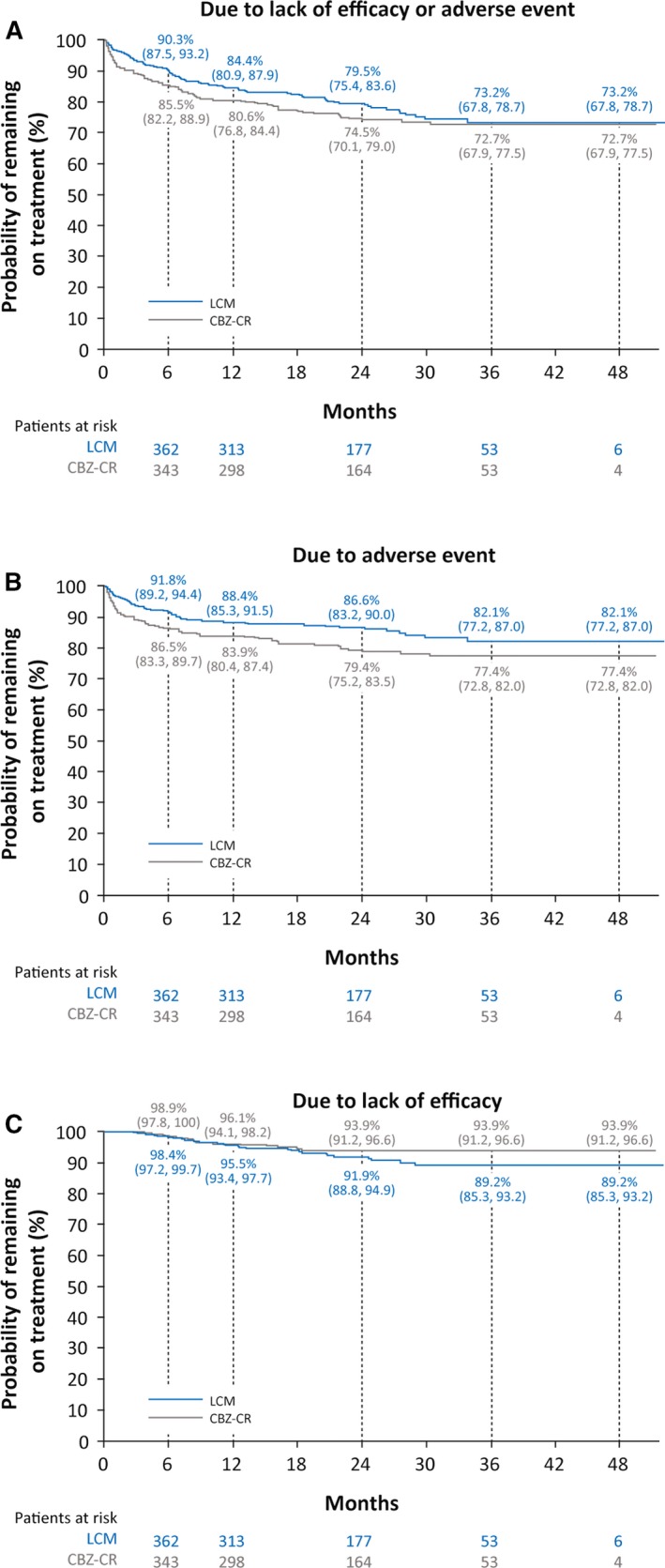
A total of 886 patients were treated in the initial trial and 548 in the extension; 211 of 279 patients (75.6%) on lacosamide and 180/269 (66.9%) on carbamazepine-CR completed the extension. In the extension, 181 patients (64.9%) on lacosamide and 182 (67.7%) on carbamazepine-CR reported TEAEs; in both groups, nasopharyngitis, headache, and dizziness were most common. Serious TEAEs were reported by 32 patients (11.5%) on lacosamide and 22 (8.2%) on carbamazepine-CR; 12 (4.3%) and 21 (7.8%) discontinued due to TEAEs. In the combined trials (median exposure: lacosamide 630 days; carbamazepine-CR 589 days), Kaplan-Meier estimated proportions of patients with 12- and 24-month seizure freedom from first dose were 50.8% (95% confidence interval 46.2%-55.4%) and 47.0% (42.2%-51.7%) on lacosamide, and 54.9% (50.3%-59.6%) and 50.9% (46.0%-55.7%) on carbamazepine-CR. Incidences of drug-related TEAEs and discontinuations due to TEAEs increased by number of comorbid conditions and were lower in patients on lacosamide.
Long-term (median ~2 years) lacosamide monotherapy was efficacious and generally well tolerated in adults with newly diagnosed epilepsy. Seizure freedom rates were similar with lacosamide and carbamazepine-CR.
一项大规模、双盲试验(SP0993;NCT01243177)表明,在疗效方面,拉科酰胺不亚于卡马西平控释剂(卡马西平-CR),并且作为新诊断为癫痫的患者的一线单药治疗,具有良好的耐受性。我们报告了非劣效性试验(SP0994;NCT01465997)的双盲扩展的主要安全性结果,以及来自两项试验的长期安全性和疗效数据的事后分析。
患者按 1:1 随机分为拉科酰胺或卡马西平-CR。根据控制癫痫发作的情况,逐渐增加剂量(拉科酰胺:200/400/600mg/d;卡马西平-CR:400/800/1200mg/d)。符合条件的患者在扩展期继续接受随机治疗。扩展期的主要结局是治疗期间出现的不良事件(TEAEs)、严重的 TEAEs 和因 TEAEs 而停药。对来自联合试验的数据的事后分析包括 12 个月和 24 个月的无癫痫发作率和根据合并症数量的 TEAEs。
共有 886 名患者在初始试验中接受治疗,548 名患者在扩展期接受治疗;拉科酰胺组有 279 名患者中的 211 名(75.6%)和卡马西平-CR 组的 269 名患者中的 180 名(66.9%)完成了扩展期。在扩展期,拉科酰胺组有 181 名患者(64.9%)和卡马西平-CR 组有 182 名患者(67.7%)报告 TEAEs;两组中最常见的 TEAEs 是鼻咽炎、头痛和头晕。拉科酰胺组有 32 名患者(11.5%)和卡马西平-CR 组有 22 名患者(8.2%)报告严重的 TEAEs;有 12 名(4.3%)和 21 名(7.8%)因 TEAEs 而停药。在联合试验中(中位暴露:拉科酰胺 630 天;卡马西平-CR 589 天),首次剂量后 12 个月和 24 个月无癫痫发作的 Kaplan-Meier 估计比例分别为拉科酰胺组 50.8%(95%置信区间 46.2%-55.4%)和 47.0%(42.2%-51.7%),卡马西平-CR 组为 54.9%(50.3%-59.6%)和 50.9%(46.0%-55.7%)。药物相关 TEAEs 的发生率和因 TEAEs 而停药的比例随着合并症数量的增加而增加,拉科酰胺组的发生率和比例较低。
在新诊断为癫痫的成人中,长期(中位~2 年)拉科酰胺单药治疗是有效且通常耐受良好的。拉科酰胺和卡马西平-CR 的无癫痫发作率相似。