Divisions of Gastroenterology and Hepatology.
Hematology and Medical Oncology, Knight Cancer Institute.
J Clin Gastroenterol. 2020 Sep;54(8):741-746. doi: 10.1097/MCG.0000000000001285.
The goal of this study was to describe potential key differences in thromboelastography (TEG) variables in hospitalized cirrhotics compared with a healthy population, identify patterns of hematologic disturbance with disease progression, and assess the value of traditional tests such as international normalized ratio (INR) and platelet count to determine coagulopathy in cirrhotics.
TEG, a functional assay of coagulation, has emerged as a useful tool for predicting bleeding risk in cirrhosis.
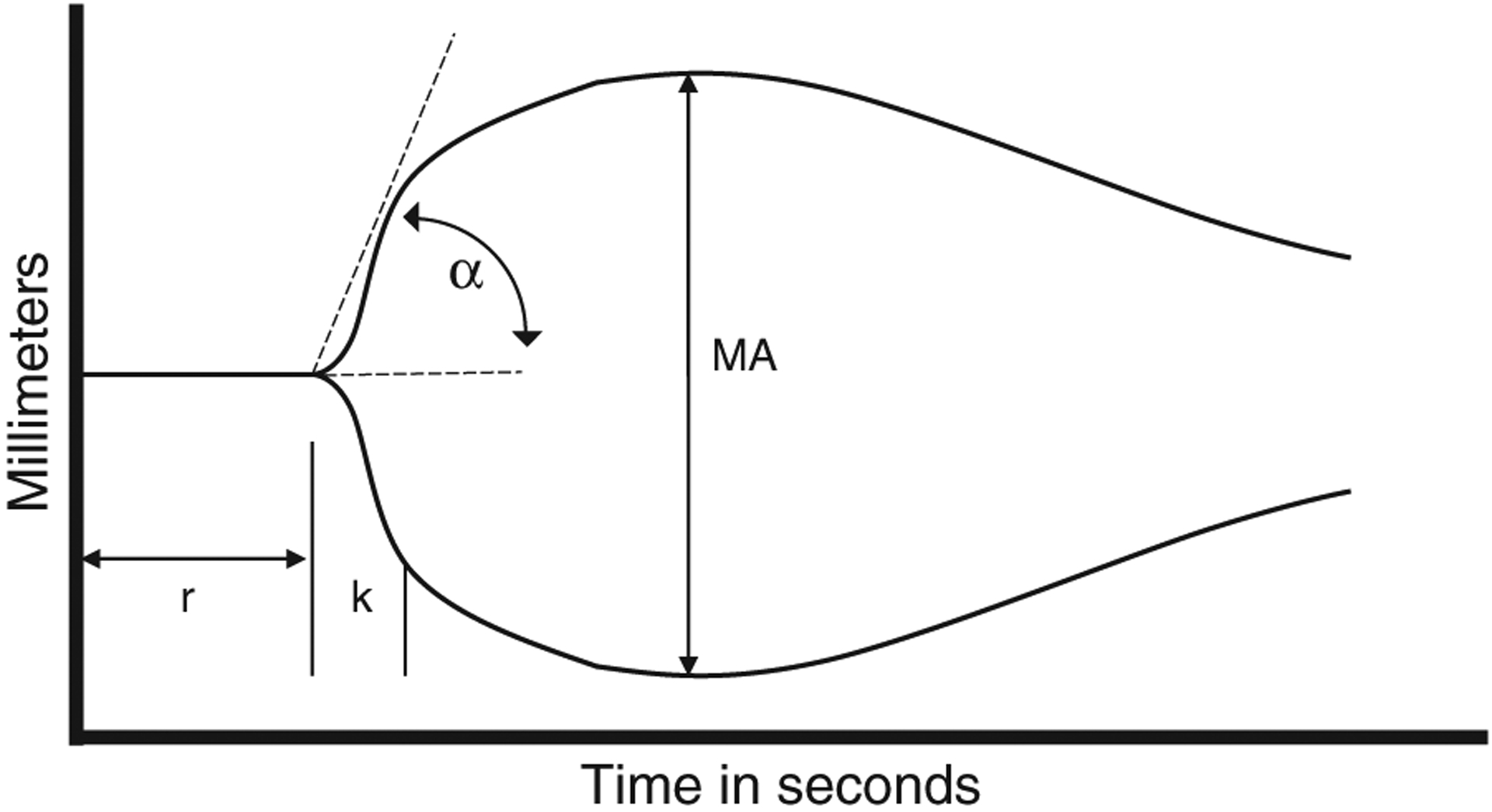
Hospitalized cirrhotics who received a TEG before any blood products between January 2017 and February 2018 at a liver transplant center were included. Reaction time (r-time), coagulation time (k-time), angle-rate of clot polymerization (α) and maximum clot strength (maximum amplitude) were measured with kaolin-activated citrated blood TEG assays.
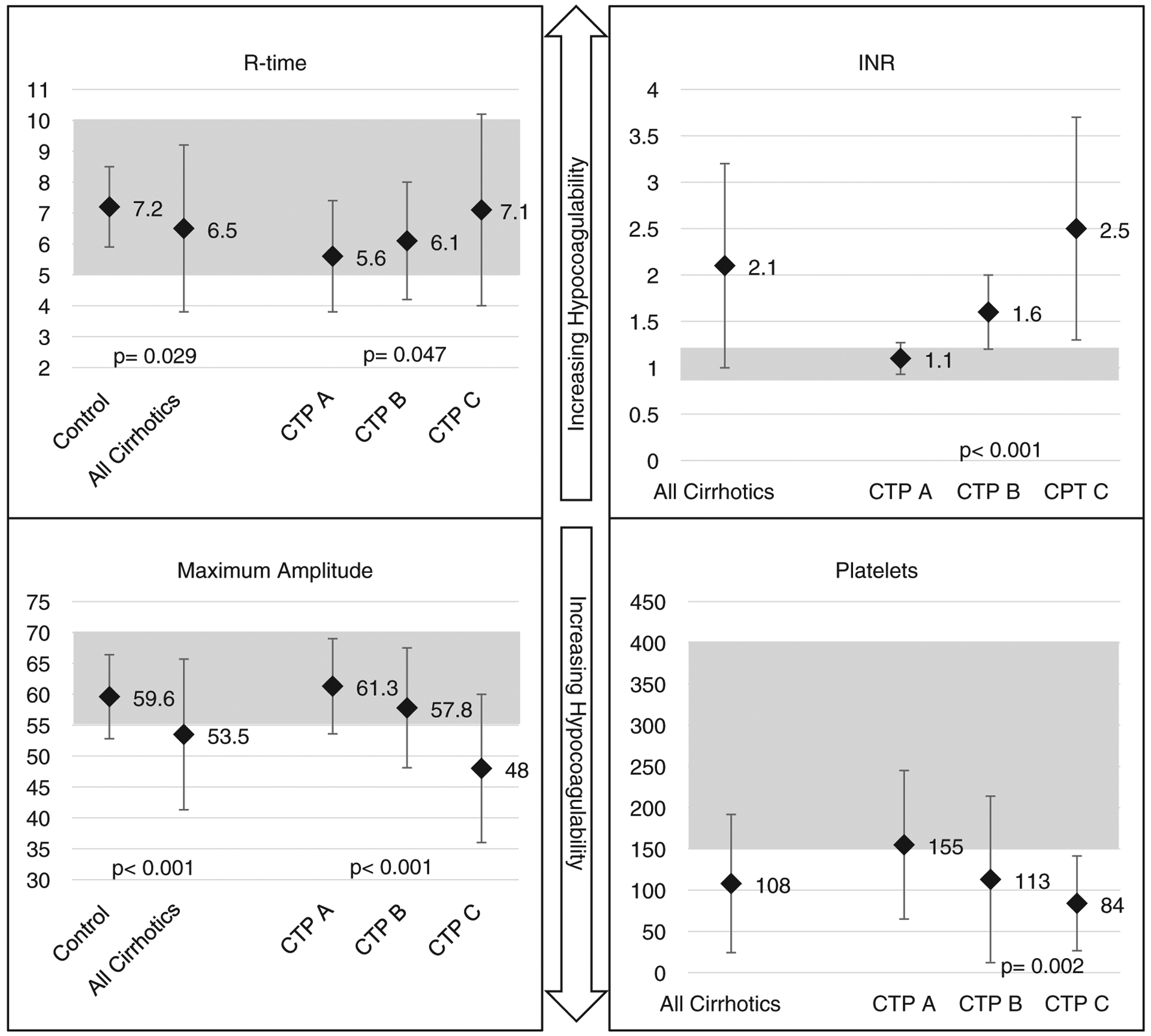
A total of 106 cirrhotic patients (Child-Turcotte-Pugh A, B, C; n=25, 25, 56) were identified for comparison against data from 53 healthy controls. TEG parameters in cirrhotics were statistically different from controls. Mean INR and platelet count for all cirrhotics were largely outside the normal reference range, contrary to TEG parameters which demonstrated parameters mostly within the normal reference ranges. The r-time, k-time, and α values in the cirrhotics progressively increased and maximum amplitude values progressively decreased as the liver disease progressed. Regression analysis showed no significant correlations between INR and r-time across any Child-Turcotte-Pugh class (r=0.01, 0.18, 0.23; P=0.95, 0.39, 0.08, respectively).
Although cirrhotics had TEG parameters within normal ranges, there was a propensity for decreased clot formation as liver function worsened. Importantly, the INR did not correlate with TEG parameters in cirrhotic patients, and given the precarious hemostatic balance in these patients, a TEG may be a better predictor of bleeding risk.
本研究旨在描述与健康人群相比,住院肝硬化患者血栓弹力图(TEG)变量的潜在关键差异,确定疾病进展过程中血液学紊乱的模式,并评估国际标准化比值(INR)和血小板计数等传统检测在确定肝硬化患者凝血功能障碍方面的价值。
TEG 是一种凝血功能的功能性检测方法,已成为预测肝硬化患者出血风险的有用工具。
本研究纳入了 2017 年 1 月至 2018 年 2 月期间在肝移植中心接受 TEG 检测且未输注任何血液制品的住院肝硬化患者。使用高岭土激活的枸橼酸盐血液 TEG 检测法测量反应时间(r-time)、凝血时间(k-time)、凝块形成速率角(α)和最大凝块强度(最大振幅)。
共确定了 106 例肝硬化患者(Child-Turcotte-Pugh A、B、C;n=25、25、56)与 53 例健康对照数据进行比较。肝硬化患者的 TEG 参数与对照组有统计学差异。所有肝硬化患者的平均 INR 和血小板计数均大大超出正常参考范围,而 TEG 参数则显示出参数大多在正常参考范围内。随着肝病的进展,肝硬化患者的 r-time、k-time 和 α 值逐渐增加,而最大振幅值逐渐降低。回归分析显示,在任何 Child-Turcotte-Pugh 分级中,INR 与 r-time 之间均无显著相关性(r=0.01、0.18、0.23;P=0.95、0.39、0.08)。
尽管肝硬化患者的 TEG 参数在正常范围内,但随着肝功能恶化,凝块形成的趋势下降。重要的是,INR 与肝硬化患者的 TEG 参数不相关,鉴于这些患者的止血平衡不稳定,TEG 可能是出血风险的更好预测指标。