Hall Teresa, Kakuma Ritsuko, Palmer Lisa, Minas Harry, Martins João, Armstrong Greg
1Nossal Institute for Global Health, University of Melbourne, 333 Exhibition St, Melbourne, VIC 3004 Australia.
2Centre for Global Mental Health, London School of Hygiene and Tropical Medicine, London, UK.
Int J Ment Health Syst. 2019 Nov 16;13:72. doi: 10.1186/s13033-019-0328-1. eCollection 2019.
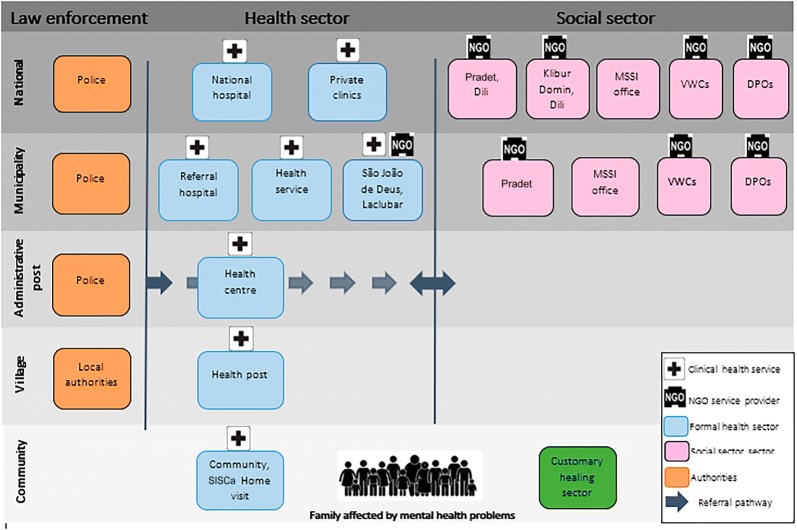
Intersectoral collaboration is fundamental to the provision of people-centred mental health care, yet there is a dearth of research about how this strategy operates within mental health systems in low- and middle-income countries. This is problematic given the known attitudinal, structural and resource barriers to intersectoral collaboration in high-income country mental health systems. This study was conducted to investigate intersectoral collaboration for people-centred mental health care in Timor-Leste, a South-East Asian country in the process of strengthening its mental health system.
This study employed a mixed-methods convergent design. Qualitative data elicited from in-depth interviews with 85 key stakeholders and document review were complemented with quantitative social network analysis to assess understandings of, the strength and structure of intersectoral collaboration in the Timorese mental health system.
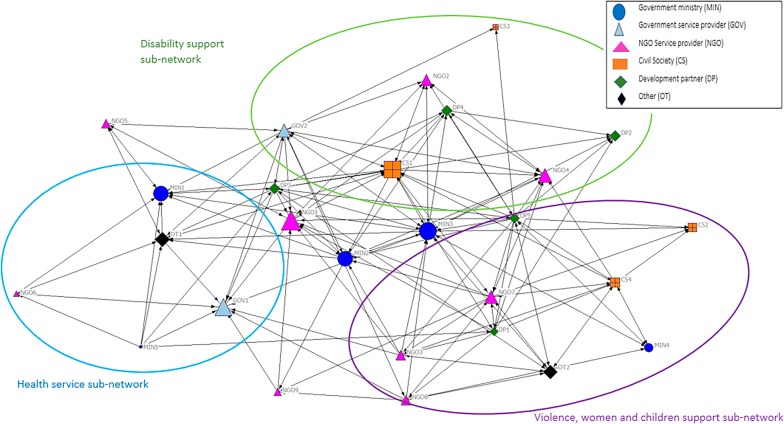
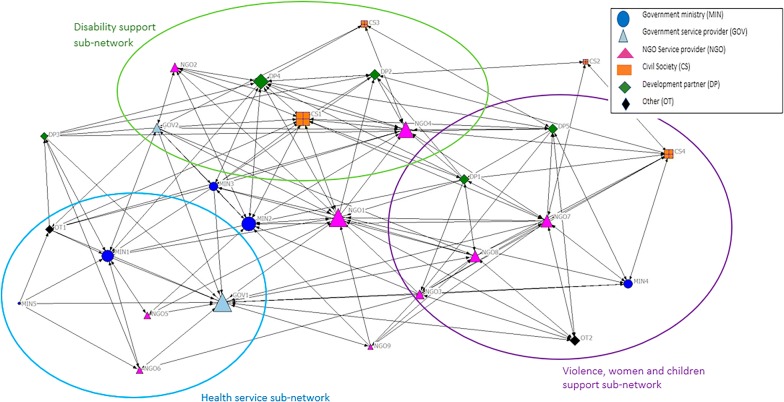
There was consensus among stakeholder groups that intersectoral collaboration for mental health is important in Timor-Leste. Despite resource restrictions discussed by participants, interview data and social network analysis revealed evidence of information and resource sharing among organisations working within the health and social (disability and violence support) sectors in Timor-Leste (network density = 0.55 and 0.30 for information and resource sharing, respectively). Contrary to the assumption that mental health services and system strengthening are led by the Ministry of Health, the mixed-methods data sources identified a split in stewardship for mental health between subnetworks in the health and social sectors (network degree centralisation = 0.28 and 0.47 for information and resource sharing, respectively).
Overall, the findings suggest that there may be opportunities for intersectoral collaborations in mental health systems in LMICs which do not exist in settings with more formalised mental health systems such as HICs. Holistic understandings of health and wellbeing, and a commitment to working together in the face of resource restrictions suggest that intersectoral collaboration can be employed to achieve people-centred mental health care in Timor-Leste.
部门间协作是提供以人为本的精神卫生保健的基础,但关于这一策略在低收入和中等收入国家精神卫生系统中的运作方式,研究却十分匮乏。鉴于高收入国家精神卫生系统中存在已知的态度、结构和资源障碍,这一问题变得愈发棘手。本研究旨在调查东帝汶(一个正在加强其精神卫生系统的东南亚国家)部门间协作以提供以人为本的精神卫生保健的情况。
本研究采用了混合方法收敛设计。通过对85名关键利益相关者进行深入访谈以及文献回顾获取定性数据,并辅以定量社会网络分析,以评估对东帝汶精神卫生系统中部门间协作的理解、强度和结构。
利益相关者群体一致认为,部门间协作对于东帝汶的精神卫生至关重要。尽管参与者讨论了资源限制,但访谈数据和社会网络分析显示,东帝汶卫生和社会(残疾与暴力支持)部门内的组织之间存在信息和资源共享的证据(信息和资源共享的网络密度分别为0.55和0.30)。与精神卫生服务和系统强化由卫生部主导的假设相反,混合方法数据源显示,卫生和社会部门的子网在精神卫生管理方面存在分歧(信息和资源共享的网络度中心性分别为0.28和0.47)。
总体而言,研究结果表明,低收入和中等收入国家的精神卫生系统中可能存在部门间协作的机会,而在高收入国家等精神卫生系统更为正规化的环境中则不存在这种机会。对健康和福祉的整体理解以及在资源限制面前共同努力的承诺表明,部门间协作可用于在东帝汶实现以人为本的精神卫生保健。