Medical Decision Making, Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, Zuid-Holland, the Netherlands.
Department of Medical Psychology, Amsterdam Public Health Research Institute, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Noord-Holland, the Netherlands.
Med Decis Making. 2020 Jan;40(1):52-61. doi: 10.1177/0272989X19889905. Epub 2019 Dec 2.
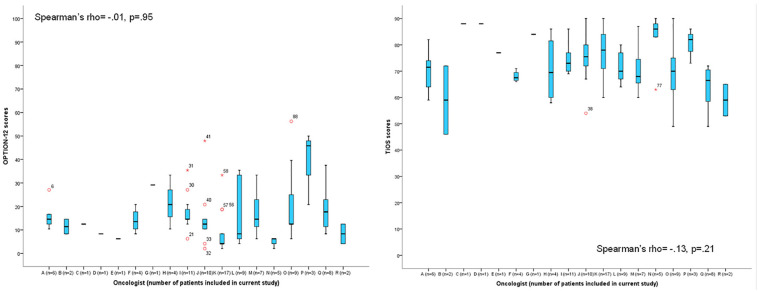
. Adjuvant systemic treatment for early stage breast cancer significantly reduces the risk of mortality but is associated with side effects, reducing patients' quality of life. Decisions about adjuvant treatment are preference sensitive and are thus ideally suited to a shared decision making (SDM) approach. Whether and how SDM affects patients' trust in their oncologist is currently unknown. We investigated the association between patients' trust in their oncologist and 1) observed level of SDM in the consultation, 2) congruence between patients' preferred and perceived level of participation, and 3) patient and oncologist characteristics. . Decision consultations ( = 101) between breast cancer patients and their medical oncologist were audio-recorded and transcribed verbatim. Patients' trust in their oncologist was measured using the Trust in Oncologist Scale (TiOS). The observed level of SDM was scored using the 12-item Observing Patient Involvement In Decision Making scale (OPTION-12), preferred level of participation with the Control Preferences Scale, and perceived level of participation with an open question in telephonic interviews. . The average TiOS score was high overall (mean [SD] = 4.1 [.56]; range, 2.6-5.0). Low levels of SDM were observed (mean [SD] = 16 [11.6]; range, 2-56). Neither observed nor perceived level of participation in SDM was associated with trust. Patients' preferred and perceived role in decision making was incongruent in almost 50% of treatment decisions. Congruence was not related to trust. A larger tumor size (β = 4.5, = 0.03) and the use of a risk prediction model during the consultation (β = 4.1, = 0.04) were associated with stronger trust. . Patients reported strong trust in their oncologist. While low levels of SDM were observed, SDM was not associated with trust. These findings suggest it may not be necessary to worry about negative consequences for trust of using SDM or risk prediction models in oncological consultations. Considering the increased emphasis on implementing SDM, it is important to further explore how SDM affects trust in clinical practice.
. 辅助全身治疗早期乳腺癌可显著降低死亡率,但与副作用有关,降低了患者的生活质量。辅助治疗决策具有偏好敏感性,因此非常适合采用共同决策(SDM)方法。SDM 是否以及如何影响患者对肿瘤医生的信任目前尚不清楚。我们调查了患者对肿瘤医生的信任与 1)咨询中观察到的 SDM 水平、2)患者偏好的参与程度和感知参与程度的一致性、3)患者和肿瘤医生的特征之间的关系。. 对 101 例乳腺癌患者及其肿瘤内科医生的决策咨询进行了录音和逐字转录。使用信任肿瘤医生量表(TiOS)测量患者对肿瘤医生的信任。使用 12 项观察患者参与决策制定量表(OPTION-12)、控制偏好量表评估偏好参与度、电话访谈中的开放问题评估感知参与度来评估 SDM 的观察水平。. TiOS 评分总体较高(平均值[标准差] = 4.1[.56];范围,2.6-5.0)。观察到的 SDM 水平较低(平均值[标准差] = 16[11.6];范围,2-56)。无论是观察到的还是感知到的 SDM 参与度都与信任无关。在近一半的治疗决策中,患者的偏好和感知决策角色不一致。一致性与信任无关。肿瘤较大(β = 4.5, = 0.03)和咨询中使用风险预测模型(β = 4.1, = 0.04)与更强的信任相关。. 患者报告对其肿瘤医生有很强的信任。尽管观察到低水平的 SDM,但 SDM 与信任无关。这些发现表明,在肿瘤学咨询中使用 SDM 或风险预测模型可能不会对信任产生负面影响,不必为此担心。考虑到越来越强调实施 SDM,重要的是要进一步探讨 SDM 在临床实践中如何影响信任。