Department of Pediatric Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, Hubei Province, China.
World J Gastroenterol. 2019 Dec 14;25(46):6781-6789. doi: 10.3748/wjg.v25.i46.6781.
A one-stage laparoscopic operation has recently been considered a favorable option for the management of patients with Hirschsprung's disease (HD) due to its superior cosmetic results. One-stage transanal endorectal pull-through for the treatment of rectosigmoid HD has been widely used in newborns without complications. However, enterostomy is required in some HD cases for enterocolitis and dilated colon. Our transumbilical enterostomy (TUE) and two-stage laparoscopy-assisted anorectoplasty were effective and achieved a similar cosmetic effect to one-stage laparoscopy on the abdominal wall in patients with anorectal malformation, but the effect in patients with HD is unclear.
To evaluate the safety, efficacy and cosmetic results of TUE in two-stage laparoscopy-assisted pull-through for HD.
From June 2013 to June 2018, 53 patients (40 boys, 13 girls; mean age at enterostomy: 5.5 ± 2.2 mo) who underwent enterostomy and two-stage laparoscopy-assisted pull-through for HD with stoma closure were reviewed at our institution. Two enterostomy approaches were used: TUE in 24 patients, and conventional abdominal enterostomy (CAE) in 29 patients. Eleven patients with rectosigmoid HD had severe preoperative enterocolitis or a dilated colon. 26 patients had long-segment HD, and 16 patients had total colonic aganglionosis (TCA). The patients with left-sided HD underwent the two-stage laparoscopic Soave procedure, and the patients with right-sided HD and TCA underwent the laparoscopic Duhamel procedure. Demographics, enterostomy operative time, complications and cosmetic results were respectively evaluated.
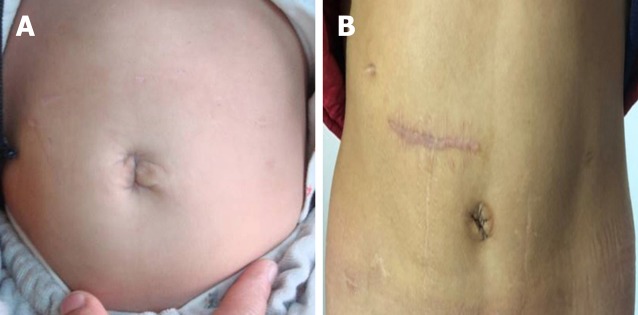
There were no differences between the groups with respect to gender, age at enterostomy, weight and clinical type ( > 0.05). No conversion to open technique was required. Two patients experienced episodes of stomal mucosal prolapse in the TUE group and 1 patient in the CAE group (8.33% 3.45%, > 0.05). No parastomal hernia was observed in either of the two groups. Wound infection at the stoma was seen in 1 case in the TUE group, and 2 cases in the CAE group (4.17% 6.90%, > 0.05). No obstruction was noted in any of the patients in the TUE group, whereas obstruction was found in 1 patient in the CAE group. Enterocolitis was observed in 3 and 5 patients in the TUE and CAE group, respectively (12.50% 17.24%, > 0.05). There was no significant difference between the TUE group and CAE group in terms of the incidence of soiling and constipation ( > 0.05). The cosmetic result using the scar score in the TUE group was better than that in the CAE group (6.83 ± 0.96 13.32 ± 1.57, < 0.05).
TUE is a safe and feasible method for the treatment of HD, and the staged enterostomy and two-stage laparoscopy-assisted pull-through achieved a similar cosmetic effect to the one-stage laparoscopic procedure.
由于腹腔镜手术具有更好的美容效果,最近被认为是治疗先天性巨结肠(HD)的一种有利选择。经肛门直肠内拖出术(Soave 手术)已广泛应用于无并发症的新生儿直肠乙状结肠型 HD 治疗,但对于并发结肠炎和结肠扩张的 HD 患者需要行肠造口术。我们的经脐肠造口术(TUE)和两阶段腹腔镜辅助肛门直肠成形术在治疗肛门直肠畸形患者时是有效且安全的,与腹壁的腹腔镜手术相比具有相似的美容效果,但在 HD 患者中的效果尚不清楚。
评估 TUE 在两阶段腹腔镜辅助 HD 经肛拖出术中的安全性、有效性和美容效果。
自 2013 年 6 月至 2018 年 6 月,我院对 53 例(男 40 例,女 13 例;肠造口术时的平均年龄:5.5±2.2 个月)接受 TUE 和两阶段腹腔镜辅助 HD 肠造口关闭术的患者进行了回顾性研究。采用两种肠造口术方式:24 例患者采用 TUE,29 例患者采用传统腹部肠造口术(CAE)。11 例患者术前存在严重的结肠炎或结肠扩张。26 例患者存在长段 HD,16 例患者存在全结肠无神经节细胞症(TCA)。左侧 HD 患者行两阶段腹腔镜 Soave 手术,右侧 HD 和 TCA 患者行腹腔镜 Duhamel 手术。分别评估患者的一般资料、肠造口术手术时间、并发症和美容效果。
两组患者在性别、肠造口术时的年龄、体重和临床类型方面无差异(>0.05)。无中转开放手术。TUE 组有 2 例患者发生吻合口黏膜脱垂,CAE 组有 1 例患者发生(8.33% 3.45%,>0.05)。两组均未发生造口旁疝。TUE 组 1 例患者发生造口感染,CAE 组 2 例患者发生(4.17% 6.90%,>0.05)。TUE 组无患者发生梗阻,CAE 组 1 例患者发生梗阻。TUE 组 3 例患者和 CAE 组 5 例患者发生结肠炎(12.50% 17.24%,>0.05)。TUE 组和 CAE 组在污粪和便秘的发生率方面无差异(>0.05)。TUE 组的美容效果评分优于 CAE 组(6.83±0.96 13.32±1.57,<0.05)。
TUE 是治疗 HD 的一种安全可行的方法,分期肠造口术和两阶段腹腔镜辅助经肛拖出术可获得与一期腹腔镜手术相似的美容效果。