Pompilio Arianna, Savini Vincenzo, Fiscarelli Ersilia, Gherardi Giovanni, Di Bonaventura Giovanni
Department of Medical, Oral and Biotechnological Sciences, and Center of Advanced Sciences and Technology (CAST), "G. d'Annunzio" University of Chieti-Pescara, Via Luigi Polacchi 11, 66100 Chieti, Italy.
Clinical Microbiology and Virology, Spirito Santo Hospital, Via Fonte Romana 8, 65124 Pescara, Italy.
Antibiotics (Basel). 2020 Jan 2;9(1):15. doi: 10.3390/antibiotics9010015.
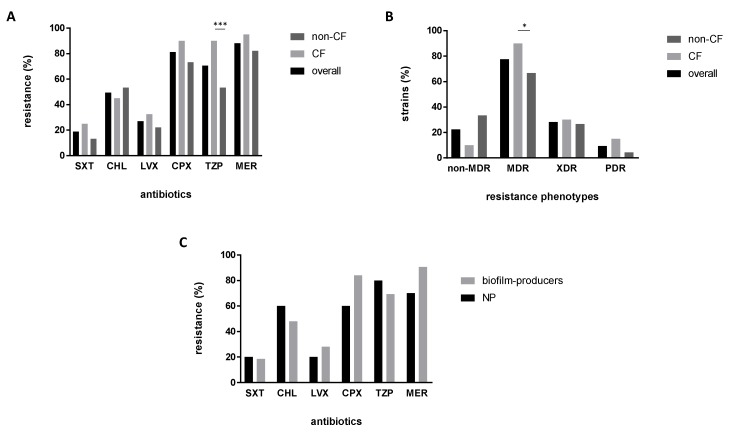
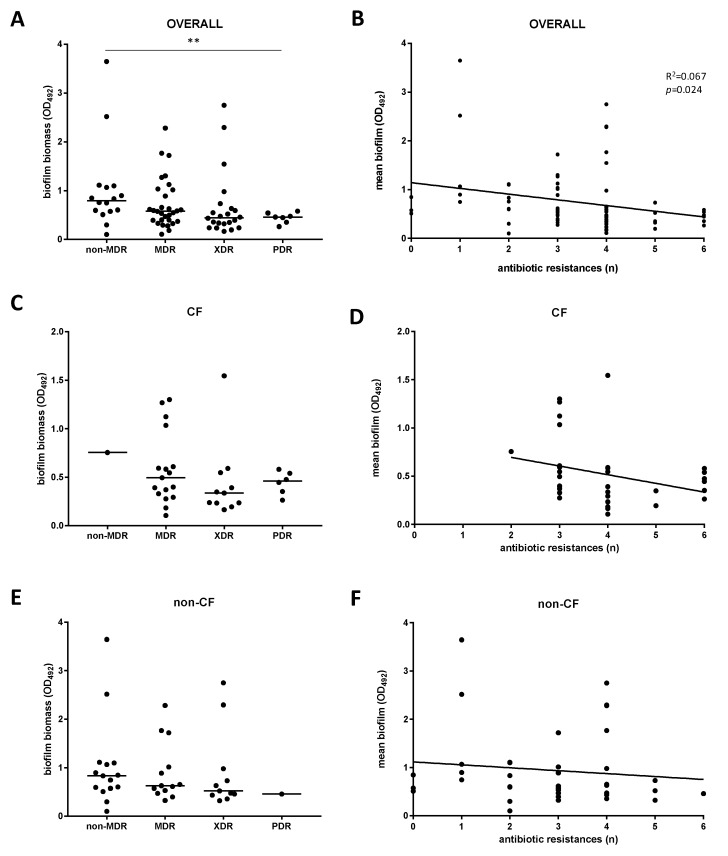
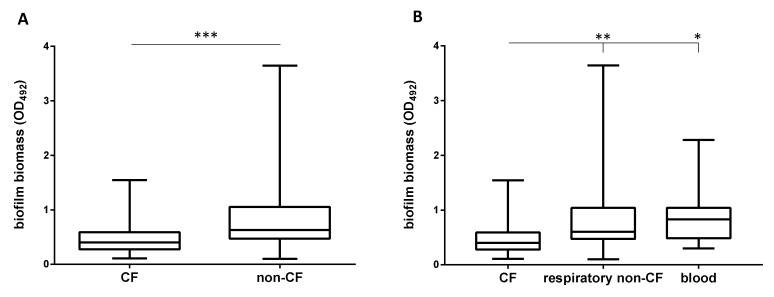
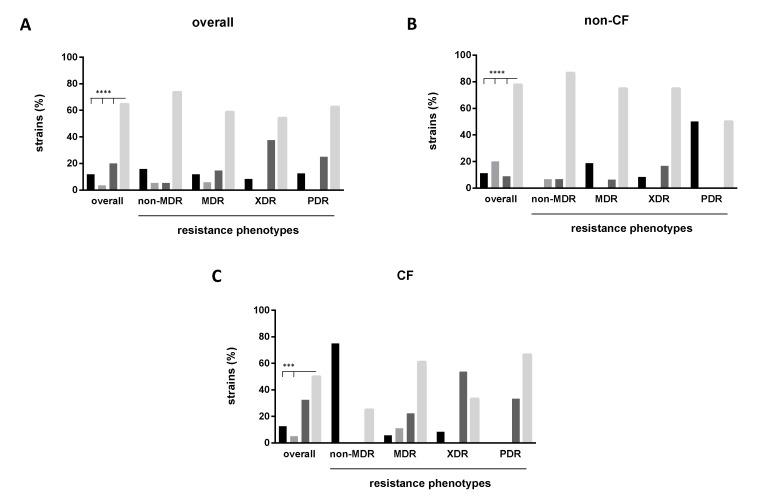
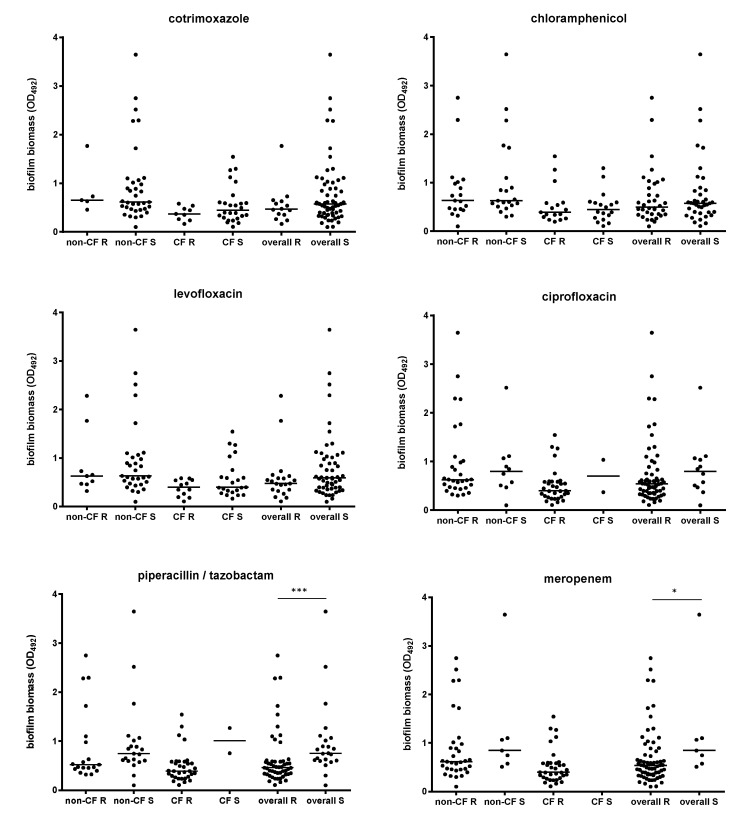
The intrinsic antibiotic resistance of , along with its ability to form biofilm both on abiotic surfaces and host tissues, dramatically affects the efficacy of the antibiotic therapy. In this work, 85 strains isolated in several hospital of central Italy and from several clinical settings were evaluated for their genetic relatedness (by pulsed-field gel electrophoresis, PFGE), biofilm formation (by microtiter plate assay), and planktonic antibiotic resistance (by Kirby-Bauer disk diffusion technique). The population showed a high genetic heterogeneity: 64 different PFGE types were identified, equally distributed in cystic fibrosis (CF) and non-CF strains, and some consisted of multiple strains. Most of the strains (88.2%) were able to form biofilm, although non-CF strains were significantly more efficient than CF strains. CF strains produced lower biofilm amounts than non-CF strains, both those from respiratory tracts and blood. Non-CF PFGE types 3 and 27 consisted of strong-producers only. Cotrimoxazole and levofloxacin were the most effective antibiotics, being active respectively against 81.2% and 72.9% of strains. CF strains were significantly more resistant to piperacillin/tazobactam compared to non-CF strains (90% versus 53.3%), regardless of sample type. Among respiratory strains, cotrimoxazole was more active against non-CF than CF strains (susceptibility rates: 86.7% versus 75%). The multidrug resistant phenotype was significantly more prevalent in CF than non-CF strains (90% versus 66.7%). Overall, the multidrug-resistance level was negatively associated with efficiency in biofilm formation. Our results showed, for the first time, that in both classical planktonic drug resistance and the ability of biofilm formation might favor its dissemination in the hospital setting. Biofilm formation might in fact act as a survival mechanism for susceptible bacteria, suggesting that clinical isolates should be routinely assayed for biofilm formation in diagnostic laboratories.
的固有抗生素耐药性,以及其在非生物表面和宿主组织上形成生物膜的能力,极大地影响了抗生素治疗的效果。在这项研究中,对从意大利中部几家医院的多个临床环境中分离出的85株菌株进行了遗传相关性评估(通过脉冲场凝胶电泳,PFGE)、生物膜形成评估(通过微量滴定板试验)和浮游菌抗生素耐药性评估(通过 Kirby-Bauer 纸片扩散技术)。该菌株群体表现出高度的遗传异质性:鉴定出64种不同的PFGE类型,在囊性纤维化(CF)和非CF菌株中均匀分布,且有些类型由多个菌株组成。大多数菌株(88.2%)能够形成生物膜,尽管非CF菌株比CF菌株形成生物膜的效率显著更高。CF菌株产生的生物膜量低于非CF菌株,无论是呼吸道来源还是血液来源的CF菌株。非CF PFGE类型3和27仅由强生物膜生产者组成。复方新诺明和左氧氟沙星是最有效的抗生素,分别对81.2%和72.9%的菌株有活性。与非CF菌株相比,CF菌株对哌拉西林/他唑巴坦的耐药性显著更高(90%对53.3%),无论样本类型如何。在呼吸道菌株中,复方新诺明对非CF菌株的活性比对CF菌株更高(敏感率:86.7%对75%)。多重耐药表型在CF菌株中比非CF菌株更为普遍(90%对66.7%)。总体而言,多重耐药水平与生物膜形成效率呈负相关。我们的结果首次表明,在医院环境中,的经典浮游菌耐药性和生物膜形成能力可能有利于其传播。生物膜形成实际上可能是敏感细菌的一种生存机制,这表明诊断实验室应常规检测临床分离株的生物膜形成情况。